Archive for the ‘News’ Category
May News
Here are some great interviews I recommend this month. Love, Mom
Leslie Manookian With Reiner Fuellmich: “People Have No Idea How Controlled Everything They See Is”
https://www.brighteon.com/348ff973-5fa6-4c20-9f79-5175dc83f6c0
CONVERSATIONS WITH DR. COWAN & FRIENDS| EP 24: LESLIE MANOOKIAN
https://www.brighteon.com/cfa5ac20-a904-4192-a527-491a1ecaf508
Great info from a large group of Doctors on the vaccines:
April News
This is one of the best articles I’ve seen on the CV vax. It’s got links to all the science. Please read and share. xo Mom
https://www.deconstructingconventional.com/post/18-reason-i-won-t-be-getting-a-covid-vaccine
18 Reasons I Won’t Be Getting a Covid Vaccine
A few friends have asked my thoughts on the covid jab(s) so I thought it was time to write an article on the topic.
All my friends had not heard most of the details I shared, so I figured you might appreciate hearing some of what I told them.
Knowing how contentious this issue is, part of me would rather just write about something else, but I feel like the discussion/news is so one-sided that I should speak up.
As I always strive to do, I promise to do my best to be level-headed and non-hysterical.
I’m not here to pick a fight with anyone, just to walk you through some of what I’ve read, my lingering questions, and explain why I can’t make sense of these covid vaccines.


THREE GROUND RULES FOR DISCUSSION
If you care to engage on this topic with me, excellent.
Here are the rules…
I am more than happy to correspond with you if…
- You are respectful and treat me the way you would want to be treated.
- You ask genuinely thoughtful questions about what makes sense to you.
- You make your points using sound logic and don’t hide behind links or the word “science.”
If you do respond, and you break any of those rules, your comments will be ignored/deleted.
With that out of the way, let me say this…
I don’t know everything, but so far no one has been able to answer the objections below.
So here are the reasons I’m opting out of the covid vaccine.
#1: VACCINE MAKERS ARE IMMUNE FROM LIABILITY
The only industry in the world that bears no liability for injuries or deaths resulting from their products, are vaccine makers.
First established in 1986 with the National Childhood Vaccine Injury Act, and reinforced by the PREP Act, vaccine makers cannot be sued, even if they are shown to be negligent.
The covid-vaccine makers are allowed to create a one-size-fits-all product, with no testing on sub-populations (i.e. people with specific health conditions), and yet they are unwilling to accept any responsibility for any adverse events or deaths their products cause.
If a company is not willing to stand behind their product as safe, especially one they rushed to market and skipped animal trials on, I am not willing to take a chance on their product.
No liability. No trust.
Here’s why…
#2: THE CHECKERED PAST OF THE VACCINE COMPANIES
The four major companies who are making these covid vaccines are/have either:
- Never brought a vaccine to market before covid (Moderna and Johnson & Johnson).
- Are serial felons (Pfizer, and Astra Zeneca).
- Are both (Johnson & Johnson).
Moderna had been trying to “Modernize our RNA” (thus the company name)–for years, but had never successfully brought ANY product to market–how nice for them to get a major cash infusion from the government to keep trying.
In fact, all major vaccine makers (save Moderna) have paid out tens of billions of dollars in damages for other products they brought to market when they knew those products would cause injuries and death–see Vioxx, Bextra, Celebrex, Thalidomide, and Opioids as a few examples.
If drug companies willfully choose to put harmful products in the market, when they can be sued, why would we trust any product where they have NO liability?
In case it hasn’t sunk in, let me reiterate…3 of the 4 covid vaccine makers have been sued for products they brought to market even though they knew injuries and deaths would result.
- Johnson & Johnson has lost major lawsuits in 1995, 1996, 2001, 2010, 2011, 2016, 2019 (For what it’s worth, J&J’s vaccine also contains tissues from aborted fetal cells, perhaps a topic for another discussion)
- Pfizer has the distinction of the biggest criminal payout in history. They have lost so many lawsuits it’s hard to count. You can check out their rap sheet here. Maybe that’s why they are demanding that countries where they don’t have liability protection put up collateral to cover vaccine-injury lawsuits.
- Astra Zeneca has similarly lost so many lawsuits it’s hard to count. Here’s one. Here’s another…you get the point. And in case you missed it, the company had their covid vaccine suspended in at least 18 countries over concerns of blood clots, and they completely botched their meeting with the FDA with numbers from their study that didn’t match.
- Oh, and apparently J&J (whose vaccine is approved for “Emergency Use” in the US) and Astrazenca (whose vaccine is not approved for “Emergency Use” in the US), had a little mix up in their ingredients…in 15 million doses. Oops.
Let me reiterate this point:
Given the free pass from liability, and the checkered past of these companies, why would we assume that all their vaccines are safe and made completely above board?
Where else in life would we trust someone with that kind of reputation?
To me that makes as much sense as expecting a remorseless, abusive, unfaithful lover to become a different person because a judge said deep down they are a good person.
No. I don’t trust them.
No liability. No trust.
Here’s another reason why I don’t trust them.
#3: THE UGLY HISTORY OF ATTEMPTS TO MAKE CORONAVIRUS VACCINES
There have been many attempts to make viral vaccines in the past that ended in utter failure, which is why we did not have a coronavirus vaccine in 2020.
In the 1960’s, scientists attempted to make an RSV (Respiratory Syncytial Virus) vaccine for infants.
In that study, they skipped animal trials because they weren’t necessary back then.
In the end, the vaccinated infants got much sicker than the unvaccinated infants when exposed to the virus in nature, with 80% of the vaccinated infants requiring hospitalization, and two of them died.
After 2000, scientists made many attempts to create coronavirus vaccines.
For the past 20 years, all ended in failure because the animals in the clinical trials got very sick and many died, just like the children in the 1960’s.
You can read a summary of this history/science here.
Or if you want to read the individual studies you can check out these links:
- In 2004 attempted vaccine produced hepatitis in ferrets
- In 2005 mice and civets became sick and more susceptible to coronaviruses after being vaccinated
- In 2012 the ferrets became sick and died. And in this study mice and ferrets developed lung disease.
- In 2016 this study also produce lung disease in mice.
The typical pattern in the studies mentioned above is that the children and the animals produced beautiful antibody responses after being vaccinated.
The manufacturers thought they hit the jackpot.
The problem came when the children and animals were exposed to the wild version of the virus.
When that happened, an unexplained phenomenon called Antibody Dependent Enhancement (ADE) also known as Vaccine Enhanced Disease (VED) occurred where the immune system produced a “cytokine storm” (i.e. overwhelmingly attacked the body), and the children/animals died.
Here’s the lingering issue…
The vaccine makers have no data to suggest their rushed vaccines have overcome that problem.
In other words, never before has any attempt to make a coronavirus vaccine been successful, nor has the gene-therapy technology that is mRNA “vaccines” been safely brought to market, but hey, since they had billions of dollars in government funding, I’m sure they figured that out.
Except they don’t know if they have…
#4: THE “DATA GAPS” SUBMITTED TO THE FDA BY THE VACCINE MAKERS
When vaccine makers submitted their papers to the FDA for the Emergency Use Authorization (Note: An EUA is not the same as a full FDA approval), among the many “Data Gaps” they reported was that they have nothing in their trials to suggest they overcame that pesky problem of Vaccine Enhanced Disease.
They simply don’t know–i.e. they have no idea if the vaccines they’ve made will also produce the same cytokine storm (and deaths) as previous attempts at such products.
As Joseph Mercola points out…
“Previous attempts to develop an mRNA-based drug using lipid nanoparticles failed and had to be abandoned because when the dose was too low, the drug had no effect, and when dosed too high, the drug became too toxic. An obvious question is: What has changed that now makes this technology safe enough for mass use?”
If that’s not alarming enough, here are other gaps in the data–i.e. there is no data to suggest safety or efficacy regarding:
- Anyone younger than age 18 or older than age 55
- Pregnant or lactating mothers
- Auto-immune conditions
- Immunocompromised individuals
- No data on transmission of covid
- No data on preventing mortality from covid
- No data on duration of protection from covid
Hard to believe right?
In case you think I’m making this up, or want to see the actual documents sent to the FDA by Pfizer and Moderna for their Emergency Use Authorization, you can check out this, or this respectively. The data gaps can be found starting with page 46 and 48 respectively.
For now let’s turn our eyes to the raw data the vaccine makers used to submit for emergency use authorization.
#5: NO ACCESS TO THE RAW DATA FROM THE TRIALS
Would you like to see the raw data that produced the “90% and 95% effective” claims touted in the news?
Me too…
But they won’t let us see that data.
As pointed out in the BMJ, something about the Pfizer and Moderna efficacy claims smells really funny.
There were “3,410 total cases of suspected, but unconfirmed covid-19 in the overall study population, 1,594 occurred in the vaccine group vs. 1,816 in the placebo group.”
Wait…what?
Did they fail to do science in their scientific study by not verifying a major variable?
Could they not test those “suspected but unconfirmed” cases to find out if they had covid?
Apparently not.
Why not test all 3,410 participants for the sake of accuracy?
Can we only guess they didn’t test because it would mess up their “90-95% effective” claims?
Where’s the FDA?
Would it not be prudent for the FDA, to expect (demand) that the vaccine makers test people who have “covid-like symptoms,” and release their raw data so outside, third-parties could examine how the manufacturers justified the numbers?
I mean it’s only every citizen of the world we’re trying to get to take these experimental products…
Why did the FDA not require that? Isn’t that the entire purpose of the FDA anyway?
Good question.
Foxes guarding the hen house?
Seems like it.
No liability. No trust.
#6: NO LONG-TERM SAFETY TESTING
Obviously, with products that have only been on the market a few months, we have no long-term safety data.
In other words, we have no idea what this product will do in the body months or years from now–for ANY population.
Given all the risks above (risks that ALL pharmaceutical products have), would it not be prudent to wait to see if the worst-case scenarios have indeed been avoided?
Would it not make sense to want to fill those pesky “data gaps” before we try to give this to every man, woman, and child on the planet?
Well…that would make sense, but to have that data, they need to test it on people, which leads me to my next point…
#7: NO INFORMED CONSENT
What most who are taking the vaccine don’t know is that because these products are still in clinical trials, anyone who gets the shot is now part of the clinical trial.
They are part of the experiment.
Those (like me) who do not take it, are part of the control group.
Time will tell how this experiment works out.
But, you may be asking, if the vaccines are causing harm, wouldn’t we be seeing that all over the news?
Surely the FDA would step in and pause the distribution?
Well, if the adverse events reporting system was working, maybe things would be different.
#8: UNDER-REPORTING OF ADVERSE REACTIONS AND DEATH
According to a study done by Harvard (at the commission of our own government), less than 1% of all adverse reactions to vaccines are actually submitted to the National Vaccine Adverse Events Reports System (VAERS) – read page 6 at the link above.
While the problems with VAERS have not been fixed (as you can read about in this letter to the CDC), at the time of this writing VAERS reports over 2,200 deaths from the current covid vaccines, as well as close to 60,000 adverse reactions.
“VAERS data released today showed 50,861 reports of adverse events following COVID vaccines, including 2,249 deaths and 7,726 serious injuries between Dec. 14, 2020 and March 26, 2021.”
And those numbers don’t include (what is currently) 578 cases of Bell’s Palsy.
If those numbers are still only 1% of the total adverse reactions (or .8 to 2% of what this study published recently in the JAMA found), you can do the math, but that equates to somewhere around 110,00 to 220,000 deaths from the vaccines to date, and a ridiculous number of adverse reactions.
Bet you didn’t see that on the news.
That death number would currently still be lower than the 424,000 deaths from medical errors that happen every year (which you probably also don’t hear about), but we are not even six months into the rollout of these vaccines yet.
If you want a deeper dive into the problems with the VAERS reporting system, you can check this out, or check this out.
But then there’s my next point, which could be argued makes these covid vaccines seem pointless…
#9: THE VACCINES DO NOT STOP TRANSMISSION OR INFECTION
Wait, what?
Aren’t these vaccines supposed to be what we’ve been waiting for to “go back to normal”?
Nope.
Why do you think we’re getting all these conflicting messages about needing to practice social distancing and wear masks AFTER we get a vaccine?
The reason is because these vaccines were never designed to stop transmission OR infection.
If you don’t believe me, I refer you again to the papers submitted to the FDA I linked to above.
The primary endpoint (what the vaccines are meant to accomplish) is to lower your symptoms.
Sounds like just about every other drug on the market right?
That’s it…lowering your symptoms is the big payoff we’ve been waiting for.
Does that seem completely pointless to anyone but me?
- It can’t stop us from spreading the virus.
- It can’t stop the virus from infecting us once we have it.
- To get the vaccine is to accept all the risk of these experimental products and the best it might do is lower symptoms?
Heck, there are plenty of other things I can do to lower my symptoms that don’t involve taking what appears to be a really risky product.
Now for the next logical question:
If we’re worried about asymptomatic spreaders, would the vaccine not make it more likely that we are creating asymptomatic spread?
If it indeed reduces symptoms, anyone who gets it might not even know they are sick and thus they are more likely to spread the virus, right?
For what it’s worth, I’ve heard many people say the side effects of the vaccine (especially the second dose) are worse than catching covid.
I can’t make sense of that either.
Take the risk.
Get no protection.
Suffer through the vaccine side-effects.
Keep wearing your mask and social distancing…
And continue to be able to spread the virus.
What?
It gets worse.
#10: PEOPLE ARE CATCHING COVID AFTER BEING FULLY VACCINATED
Talk about a bummer.
You get vaccinated and you still catch covid.
- It’s happening in Washington State
- It’s happening in New York
- It’s happening in Michigan
- It’s happening in Hawaii
- It’s happening in several other states too.
- It happened to 80% of 35 nuns who got the vaccine in Kentucky. Two of them died by the way.
In reality, this phenomenon is probably happening everywhere, but those are the ones making the news now.
Given the reasons above (and what’s below), maybe this doesn’t surprise you, but bummer if you thought the vaccine was a shield to keep you safe.
It’s not.
That was never the point.
If 66% of healthcare workers in L.A. are going to delay or skip the vaccine…maybe they aren’t wowed by the rushed science either.
Maybe they are watching the shady way deaths and cases are being reported…
#11: THE OVERALL DEATH RATE FROM COVID
According to the CDC’s own numbers, covid has a 99.74% survival rate.
Why would I take a risk on a product, that doesn’t stop infection or transmission, to help me overcome a cold that has a .26% chance of killing me–actually in my age range is has about a .1% chance of killing me (and .01% chance of killing my kids), but let’s not split hairs here.
With a bar (death rate) that low, we will be in lockdown every year…i.e. forever.
But wait, what about the 500,000 plus deaths, that’s alarming right?
I’m glad you asked.
#12: THE BLOATED COVID DEATH NUMBERS
Something smells really funny about this one.
Never before in the history of death certificates has our own government changed how deaths are reported.
Why now, are we reporting everyone who dies with covid in their body, as having died of covid, rather than the co-morbidities that actually took their life?
Until covid, all coronaviruses (common colds) were never listed as the primary cause of death when someone died of heart disease, cancer, diabetes, auto-immune conditions, or any other major co-morbidity.
The disease was listed as the cause of death, and a confounding factor like flu or pneumonia was listed on a separate line.
To bloat the number even more, both the W.H.O. and the C.D.C. changed their guidelines such that those who are suspected or probable (but were never confirmed) of having died of covid, are also included in the death numbers.
Seriously?
If we are going to do that then should we not go back and change the numbers of all past cold and flu seasons so we can compare apples to apples when it comes to death rates?
According to the CDCs own numbers, (scroll down to the section “Comorbidities and other conditions”) only 6% of the deaths being attributed to covid are instances where covid seems to be the only issue at hand.
In other words, reduce the death numbers you see on the news by 94% and you have what is likely the real numbers of deaths from just covid.
Even if the former CDC director is correct and covid-19 was a lab-enhanced virus (see Reason #14 below), a .26% death rate is still in line with the viral death rate that circles the planet ever year.
Then there’s this Fauci guy.
I’d really love to trust him, but besides the fact that he hasn’t treated one covid patient…you should probably know…
#13: FAUCI AND SIX OTHERS AT NIAID OWN PATENTS IN THE MODERNA VACCINE
Thanks to the Bayh-Dole Act, government workers are allowed to file patents on any research they do using tax payer funding.
Tony Fauci owns over 1,000 patents (see this video for more details), including patents being used on the Moderna vaccine…which he approved government funding for.
In fact, the NIH (which NIAID is part of) claims joint ownership of Moderna’s vaccine.
Does anyone else see this as a MAJOR conflict of interest, or criminal even?
I say criminal because there’s also this pesky problem that makes me even more distrustful of Fauci, NIAD, and the NIH in general.
#14: FAUCI IS ON THE HOT SEAT FOR ILLEGAL GAIN-OF-FUNCTION RESEARCH
What is “Gain-of-Function” research?
It’s where scientists attempt to make viruses gain functions–i.e. make them more transmissible and deadlier.
Sounds at least a touch unethical, right?
How could that possibly be helpful?
Our government agreed, and banned the practice.
So what did the Fauci-led NIAID do?
They pivoted and outsourced the gain-of-function research (in coronaviruses no less) to China–to the tune of a $600K grant.
You can see more details, including the important timeline of these events in this fantastically well-researched documentary.
Mr. Fauci, you have some explaining to do…and I hope the cameras are recording when you have to defend your actions.
For now, let’s turn our attention back to the virus…
#15: THE VIRUS CONTINUES TO MUTATE
Not only does the virus (like all viruses) continue to mutate, but according to world-renowned vaccine developer Geert Vanden Bossche (who you’ll meet below if you don’t know him) it’s mutating about every 10 hours.
How in the world are we going to keep creating vaccines to keep up with that level of mutation?
We’re not.
Might that also explain why fully vaccinated people are continuing to catch covid?
Why, given that natural immunity has never ultimately failed humanity, do we suddenly not trust it?
Why, if I ask questions like the above, or post links like what you find above, will my thoughts be deleted from all major social media platforms?
That brings me to the next troubling problem I have with these vaccines.
#16: CENSORSHIP…AND THE COMPLETE ABSENCE OF SCIENTIFIC DEBATE
I can’t help but get snarky here, so humor me.
How did you enjoy all those nationally and globally-televised, robust debates put on by public health officials, and broadcast simultaneously on every major news station?
Wasn’t it great hearing from the best minds in medicine, virology, epidemiology, economics, and vaccinology from all over the world as they vigorously and respectfully debated thingslike:
- Lockdowns
- Mask wearing
- Social-distancing
- Vaccine efficacy and safety trials
- How to screen for susceptibility to vaccine injury
- Therapeutics, (i.e. non-vaccine treatment options)
Wasn’t it great seeing public health officials (who never treated anyone with covid) have their “science” questioned.
Wasn’t it great seeing the FDA panel publicly grill the vaccine makers in prime time as they stood in the hot-seat of tough questions about products of which they have no liability?
Oh, wait…you didn’t see those debates?
No, you didn’t…because they never happened.
What happened instead was heavy-handed censorship of all but one narrative.
Ironically, Mark Zuckerberg can question vaccine safety, but I can’t?
Hypocrite?
When did the first amendment become a suggestion?
It’s the FIRST amendment Mark–the one our founders thought was most important.
With so much at stake, why are we fed only one narrative…shouldn’t many perspectives be heard and professionally debated?
WHAT HAS HAPPENED TO SCIENCE?
What has happened to the scientific method of always challenging our assumptions?
What happened to lively debate in this country, or at least in Western society?
Why did anyone who disagrees with the WHO, or the CDC get censored so heavily?
Is the science of public health a religion now, or is science supposed to be about debate?
If someone says “the science is settled” that’s how I know I’m dealing with someone who is closed minded.
By definition science (especially biological science) is never settled.
If it was, it would be dogma, not science.
OK, before I get too worked up, let me say this…
I WANT TO BE A GOOD CITIZEN
I really do.
If lockdowns work, I want to do my part and stay home.
If masks work, I want to wear them.
If social distancing is effective, I want to comply.
But, if there is evidence they don’t (masks for example), I want to hear that evidence too.
If highly-credentialed scientists have different opinions, I want to know what they think.
I want a chance to hear their arguments and make up my own mind.
I don’t think I’m the smartest person in the world, but I think I can think.
Maybe I’m weird, but if someone is censored, then I REALLY want to hear what they think.
Don’t you?
To all my friends who don’t have a problem with censorship, will you have the same opinion when what you think is censored?
Is censorship not the technique of dictators, tyrants, and greedy, power-hungry people?
Is it not a sign that those who are doing the censoring know it’s the only way they can win?
What if a man who spent his entire life developing vaccines was willing to put his entire reputation on the line and call on all global leaders to immediately stop the covid vaccines because of problems with the science?
What if he pleaded for an open-scientific debate on a global stage?
Would you want to hear what he has to say?
Would you want to see the debate he’s asking for?
#17: THE WORLD’S LEADING VACCINOLOGIST IS SOUNDING THE ALARM…
Here is what may be the biggest reason this covid vaccine doesn’t make sense to me.
When someone who is very pro-vaccine, who has spent his entire professional career overseeing the development of vaccines, is shouting from the mountaintops that we have a major problem, I think the man should be heard.
In case you missed it, and in case you care to watch it, here is Geert Vanden Bossche, explaining:
- Why the covid vaccine may be putting so much pressure on the virus that we are accelerating it’s ability to mutate and become more deadly.
- Why the covid vaccines may be creating vaccine-resistant viruses (similar to anti-biotic resistant bacteria).
- Why, because of previous problems with Antibody Dependent Enhancement, we may be looking at a mass casualty event in the next few months/years.
If you want to see/read about a second, and longer, interview with Vanden Bossche, where he was asked some tough questions, you can check this out.
If half of what he says comes true, these vaccines could be the worst invention of all time.
If you don’t like his science, take it up with him.
I’m just the messenger.
But I can also speak to covid personally.
#18: I ALREADY HAD COVID
I didn’t enjoy it.
It was a nasty cold for two days:
- Unrelenting butt/low-back aches
- Very low energy.
- Low-grade fever.
It was weird not being able to smell anything for a couple days.
A week later, coffee still tasted a little “off.”
But I survived.
Now it appears (as it always has) that I have beautiful, natural, life-long immunity…
…not something likely to wear off in a few months if I get the vaccine.
In my body, and my household, covid is over.
In fact, now that I’ve had it, there is evidence the covid vaccine might actually be more dangerous for me.
That is not a risk I’m willing to take.
IN SUMMARY
The above are just my reasons for not wanting the vaccine.
Maybe my reasons make sense to you, maybe they don’t.
Whatever does makes sense to you, hopefully we can still be friends.
I for one think there’s a lot more that we have in common than what separates us.
- We all want to live in a world of freedom.
- We all want to do our part to help others and to live well.
- We all want the right to express our opinions without fearing we’ll be censored or viciously attacked.
- We all deserve to have the access to the facts so we can make informed decisions.
Agree or disagree with me; I’ll treat you no differently.
You’re a human just as worthy of love and respect as anyone else.
For that I salute you, and I truly wish you all the best.
I hope you found this helpful.
If so, feel free to share.
If not, feel free to (kindly) let me know what didn’t make sense to you and I’d be happy to hear your thoughts too.
Stay curious and stay humble.
Until next time,
Christian
March News

Couldn’t resist! LOL. So much going on. I hope you all are well, in these crazy times. Never stop fighting for your freedom! Mom
Excellent interview by Reinette Senum with Dr. Sherry Tenpenny. This March 2021 update gives step by step explanations of the Covid inoculations– what most medical professionals, and public health department directors either don’t know, or aren’t telling you. Dr Sherri Tenpenny break…Lots of very important info.
Interview by Robert F Kennedy, Jr. with Naomi Wolf. In the latest episode of “TRUTH” with Robert F. Kennedy, Jr., Kennedy sat down with the iconic Naomi Wolf for a spirited discussion on abuse of power, standing up to tyranny and preserving our Constitution. Wolf explained how tyrants always follow the same predictable route in their attempts to bring democracies to a close and how she believes our society has reached “Step 10” of her “Fascism in 10 Easy Steps.”
This last link is also very interesting. Geert Vanden Bossche PhD, is an internationally recognised vaccine developer having worked as the head of the Vaccine Development Office at the German Centre for Infection Research. Coordinated Global Alliance for Vaccines and Immunisation’s Ebola Vaccine Program and contributed to the implementation of an integrated vaccine work plan in collaboration with Global Health Partners (WHO, Bill & Melinda Gates Foundation, CDC, UNICEF), regulators (FDA) and vaccine manufacturers to enable timely deployment or stockpiling of Ebola vaccine candidates. Highlighting the principle of using a prophylactic vaccine in the midst of a pandemic. Likely to create more more viral variants in the process. Sharing his perspective on mass vaccination in COVID-19.
February News
Some great info out there, being censored as usual. If they are fighting so hard to censor it – it usually is the truth. Mom
Children’s Health Defense has a great new video, The CV vaccine on trial. It’s got great speakers and is really worth watching. You can see it here:
If you are looking for links to ALL of the adverse effect including miscarriages and deaths after the experimental shot, these two sites are great.
January 2021
Is it really a ‘Vaccine’

Where to start this month… They rolled out the ‘vaccine’ it’s not even licensed by the FDA yet. It’s an experimental technology, not even actually a ‘vaccine’ it’s gene therapy. Traditional vaccines like measles have a bit of the virus so that in principle your body can develop some immunity. This covid treatment is not that.
Dr. David Martin from the January 5, 2021 Focus on Fauci event that you need to share with everyone:
Let’s make sure we are clear… This is not a vaccine. They are using the term “vaccine” to sneak this thing under public health exemptions. This is not a vaccine.
This is mRNA packaged in a fat envelope that is delivered to a cell. It is a medical device designed to stimulate the human cell into becoming a pathogen creator. It is not a vaccine. Vaccines actually are a legally defined term under public health law; they are a legally defined term under CDC and FDA standards.[1] And the vaccine specifically has to stimulate both the immunity within the person receiving it and it also has to disrupt transmission.
And that is not what this is. They (Moderna and Pfizer) have been abundantly clear in saying that the mRNA strand that is going into the cell is not to stop the transmission, it is a treatment. But if it was discussed as a treatment, it would not get the sympathetic ear of public health authorities because then people would say, “What other treatments are there?”
The use of the term vaccine is unconscionable for both the legal definition and also it is actually the sucker punch to open and free discourse… Moderna was started as a chemotherapy company for cancer, not a vaccine manufacturer for SARSCOV2. If we said we are going to give people prophylactic chemotherapy for the cancer they don’t yet have, we’d be laughed out of the room because it’s a stupid idea. That’s exactly what this is. This is a mechanical device in the form of a very small package of technology that is being inserted into the human system to activate the cell to become a pathogen manufacturing site.
And I refuse to stipulate in any conversations that this is in fact a vaccine issue. The only reason why the term is being used is to abuse the 1905 Jacobson case that has been misrepresented since it was written. And if we were honest with this, we would actually call it what it is: it is a chemical pathogen device that is actually meant to unleash a chemical pathogen production action within a cell. It is a medical device, not a drug because it meets the CDRH definition of a device. It is not a living system, it is not a biologic system, it is a physical technology – it happens to just come in the size of a molecular package.
So, we need to be really clear on making sure we don’t fall for their game. Because their game is if we talk about it as a vaccine then we are going to get into a vaccine conversation but this is not, by their own admission, a vaccine. As a result it must be clear to everyone listening that we will not fall for this failed definition just like we will not fall for their industrial chemical definition of health. Both of them are functionally flawed and are an implicit violation of the legal construct that is being exploited. I get frustrated when I hear activists and lawyers say, “we are going to fight the vaccine”. If you stipulate it’s a vaccine you’ve already lost the battle. It’s not a vaccine. It is made to make you sick.
80% of the people exposed to SARSCOV2 are asymptomatic carriers. 80% of people who get this injected into them experience a clinical adverse event. You are getting injected with a chemical substance to induce illness, not to induce an immuno-transmissive response. In other words, nothing about this is going to stop you from transmitting anything. This is about getting you sick and having your own cells be the thing that get you sick.
When the paymaster for the distribution of information happens to be the industry that’s doing the distributing, we lose. Because the only narrative is the one that will be compensated by the people writing the check. That goes for our politicians… and our media – it has been paid for – if you follow the money you realize there is no non-conflicted voice on any network.[1] The word “vaccine” originates from the Latin Variolae vaccinae (cowpox), which Edward Jenner demonstrated in 1798 could prevent smallpox in humans. Today the term ‘vaccine’ applies to all biological preparations, produced from living organisms, that enhance immunity against disease and either prevent (prophylactic vaccines) or, in some cases, treat disease (therapeutic vaccines). From: http://www.phrma-jp.org/wordpress/wp-content/uploads/old/library/vaccine-factbook_e/1_Basic_Concept_of_Vaccination.pdf
‘This Week’ With Mary + Polly: You Can’t Sweep Deaths Under the Rug + Free Pot With Your COVID Shot? + More
In “This Week” with Mary Holland, Children’s Health Defense vice chair and general counsel, and Polly Tommey, co-producer of “Vaxxed,” Mary and Polly discuss the growing reports of injuries and deaths from COVID vaccines … and more. Read more here,
Side Effects and Data Gaps Raise Questions on COVID Vaccine
- Reports of serious side effects to the COVID-19 vaccines have started emerging. Examples include persistent malaise and extreme exhaustion, anaphylactic reactions, multisystem inflammatory syndrome, chronic seizures and convulsions, paralysis and sudden death within hours or days
- By December 18, 2020, 112,807 Americans had received their first dose of COVID-19 vaccine. Of those, 3,150 suffered one or more “health impact events.” That’s a side effect rate of 2.79%
- While Pfizer claims its vaccine is 95% effective, this is the relative risk reduction. The absolute risk reduction is actually less than 1%
- Analysis of recently released data suggests the relative risk reduction for Pfizer’s vaccine may actually be between 19% and 29% — far lower than the required licensing threshold of 50%
- Studies have warned COVID-19 vaccines may result in more serious disease when exposed to the virus, either through antibody-dependent immune enhancement or pathogen priming that triggers an autoimmune response
- Read more here, https://articles.mercola.com/sites/articles/archive/2021/01/26/covid-vaccine-side-effects.aspx
Here is a link for a site that is reporting all adverse effects occurring around the world, https://hpv-vaccine-side-effects.com/covid-19-vaccine-side-effects-world-map/
WHO, Fauci Warn COVID-19 Vaccines May Not Prevent Infection and Disease Transmission
At a virtual press conference held by the World Health Organization (WHO) on Dec. 28, 2020, WHO officials warned there is no guarantee that COVID-19 vaccines will prevent people from being infected with the SARS-CoV-2 virus and transmitting it to other people.1 In a New Year’s Day interview with Newsweek, Anthony Fauci, MD, Director of the National Institute of Allergy and Infectious Diseases (NIAID), reinforced the WHO’s admission that health officials do not know if COVID-19 vaccines prevent infection or if people can spread the virus to others after getting vaccinated.2 According to U.S. and WHO health officials, vaccinated persons still need to mask and social distance because they could be able to spread the new coronavirus to others without knowing it.3 4
Although the U.S. Food and Drug Administration (FDA) granted Emergency Use Authorization (EUA) in December 2020 for Pfizer/BioNTech5 and Moderna6 to release their experimental mRNA vaccines for use in the U.S., the companies only provided evidence from clinical trials to demonstrate that their vaccines prevented more mild to severe COVID-19 disease symptoms in vaccinated participants compared to unvaccinated trial participants. The companies did not investigate whether the vaccines prevent people from becoming asymptomatically infected with the SARS-CoV-2 virus and/or transmitting it to other people.7 8 Read more here, https://thevaccinereaction.org/2021/01/who-fauci-warn-covid-19-vaccines-may-not-prevent-infection-and-disease-transmission/
Oracle Films, a Bristol-based production company, has released a video called Ask The Experts (Covid-19 Vaccine), uploaded on 7 December.
The video, made in collaboration with Fiona Hine, Founder of CoviLeaks, features 33 Doctors and a few other professionals – including some names you’ll be familiar with and others you won’t – who all urge caution regarding the CV-19 vaccine. This is a great video, watch here, https://off-guardian.org/2020/12/09/watch-ask-the-experts-covid-19-vaccine/
December 2020
Some links and news. Wishing everyone a happy and healthy holiday season. Mom
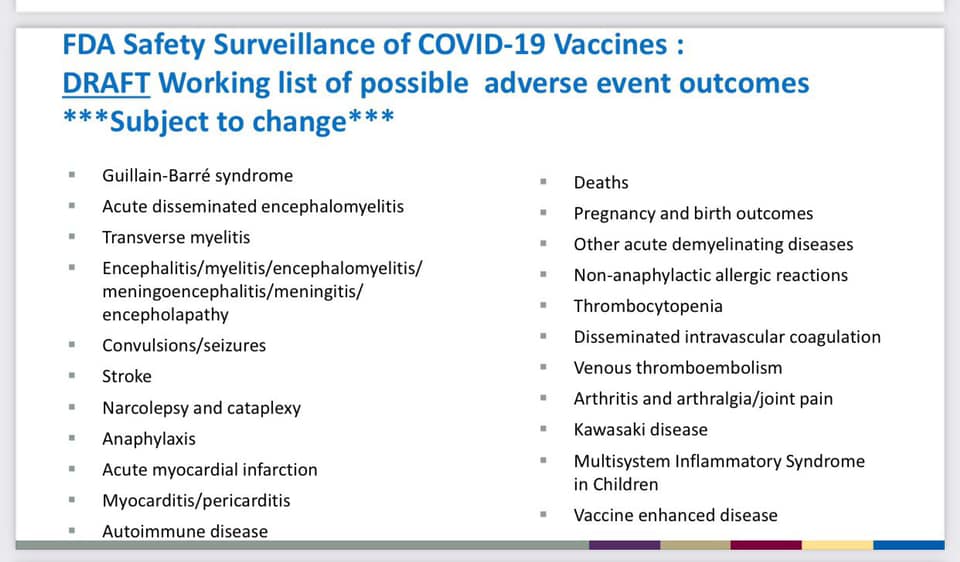
The above is a list of possible side effects from the CV vac – No animal tests, no long term testing, no independent testing.
The Coronavirus Vaccine Uncensored | Robert F. Kennedy Jr. & Del Bigtree
The wonderful Brandy Vaughn, from LearnTheRisk.org was found dead this week. Please support her fundraiser, if you’re able.
https://gogetfunding.com/in-honor-of-brandy-vaughan-learntherisk/
The Highwire with Del Bigtree did an excellent Vaccine Safety presentation a few weeks back. Really worth watching and sharing. Click on the link below.
Here’s what happened the last time we rushed a vaccine.
September News
Here’s the best of the recent news. Love, Mom
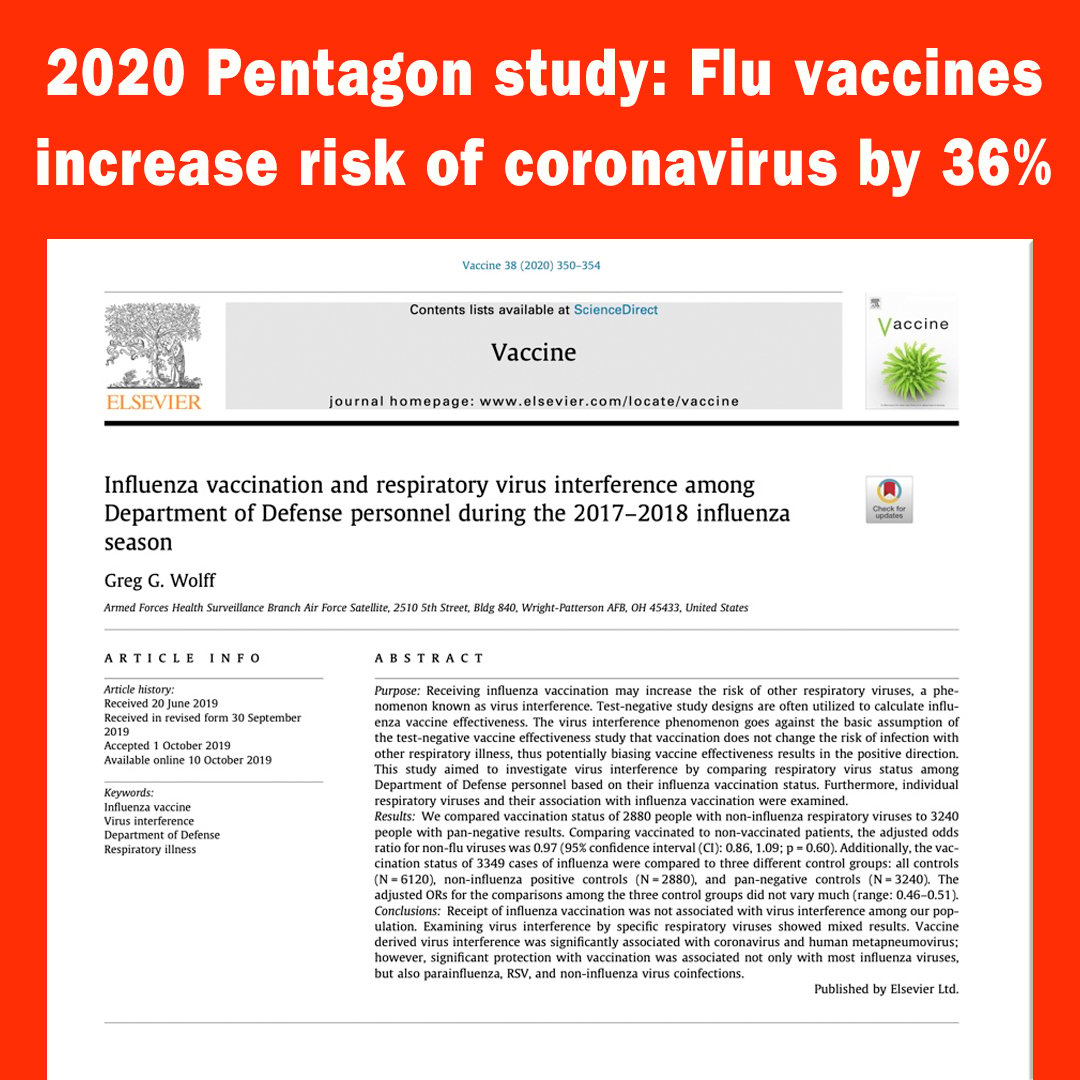
Pentagon Study: Flu Shot Raises Risk of Coronavirus by 36% (and Other Supporting Studies)
By Robert F. Kennedy, Jr., Chairman, Children’s Health Defense
On March 12th, 2020, Anderson Cooper and Dr. Sanjay Gupta held a global town hall on “Corona Facts and Fears.” During the discussion, Anderson said to the viewing audience, “And, again, if you are concerned about coronavirus, and you haven’t gotten a flu shot…you should get a flu shot.”
Setting safety and efficacy of influenza vaccination aside, is Anderson’s claim that the flu shot will help people fight COVID-19 remotely true? The short answer is no.
In fact, the results of many peer-reviewed, published studies prove that Anderson’s recommendation may have been the worst advice he could have given the public.
In searching the literature, the only study we have been able to find assessing flu shots and coronavirus is a 2020 US Pentagon study that found that the flu shot INCREASES the risks from coronavirus by 36%. “Receiving influenza vaccination may increase the risk of other respiratory viruses, a phenomenon known as “virus interference…’vaccine derived’ virus interference was significantly associated with coronavirus…” Here are the findings:
2020 Pentagon study: Flu vaccines increase risk of coronavirus by 36%
Examining non-influenza viruses specifically, the odds of coronavirus in vaccinated individuals were significantly higher when compared to unvaccinated individuals with an odds ratio (association between an exposure and an outcome) of 1.36. In other words, the vaccinated were 36% more likely to get coronavirus.

Many other studies suggest the increased risk of viral respiratory infections from the flu shot:
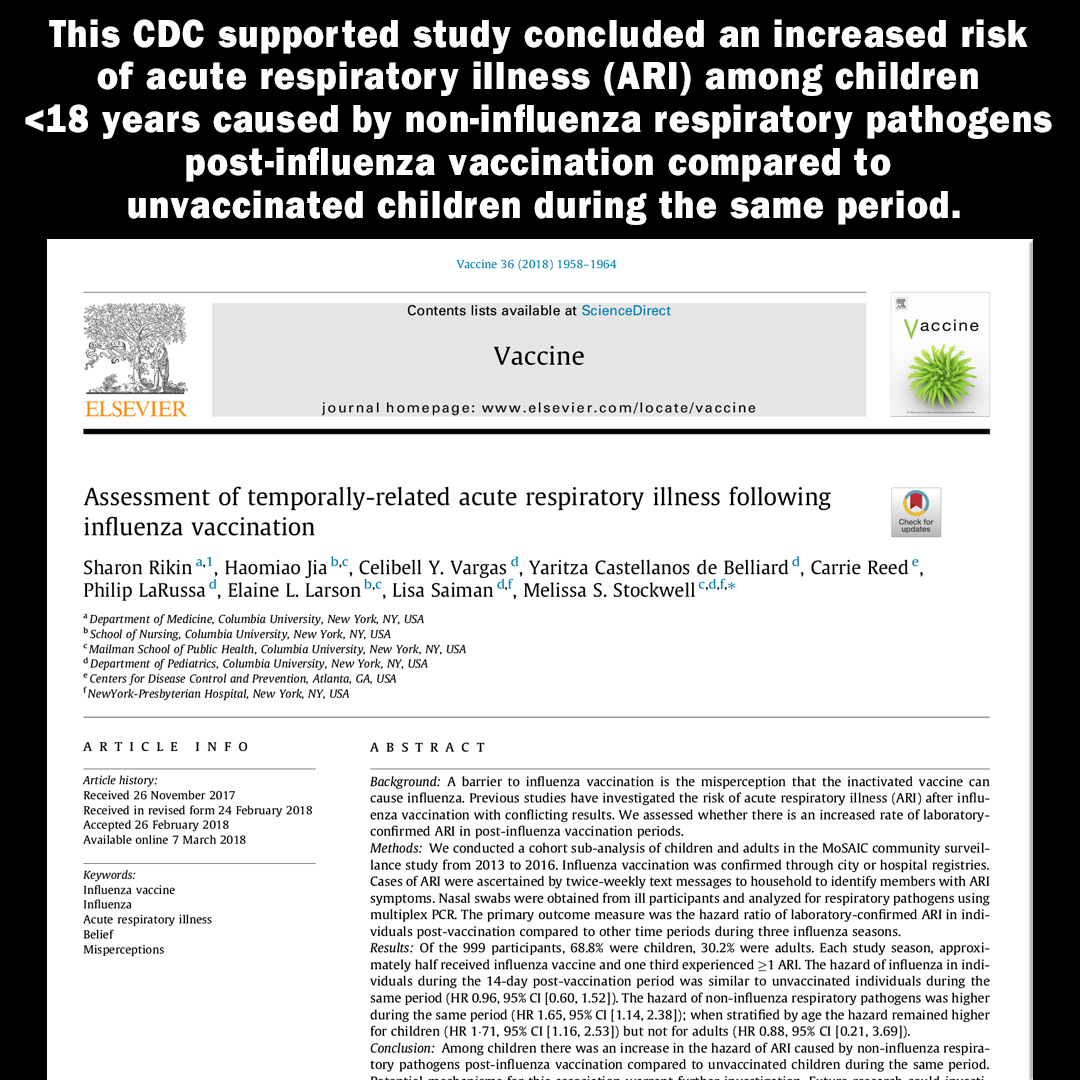
2018 CDC Study: Flu shots increase risk of non-flu acute respiratory illnesses (ARI) in children.
This CDC supported study concluded an increased risk of acute respiratory illness (ARI) among children <18 years caused by non-influenza respiratory pathogens post-influenza vaccination compared to unvaccinated children during the same period.

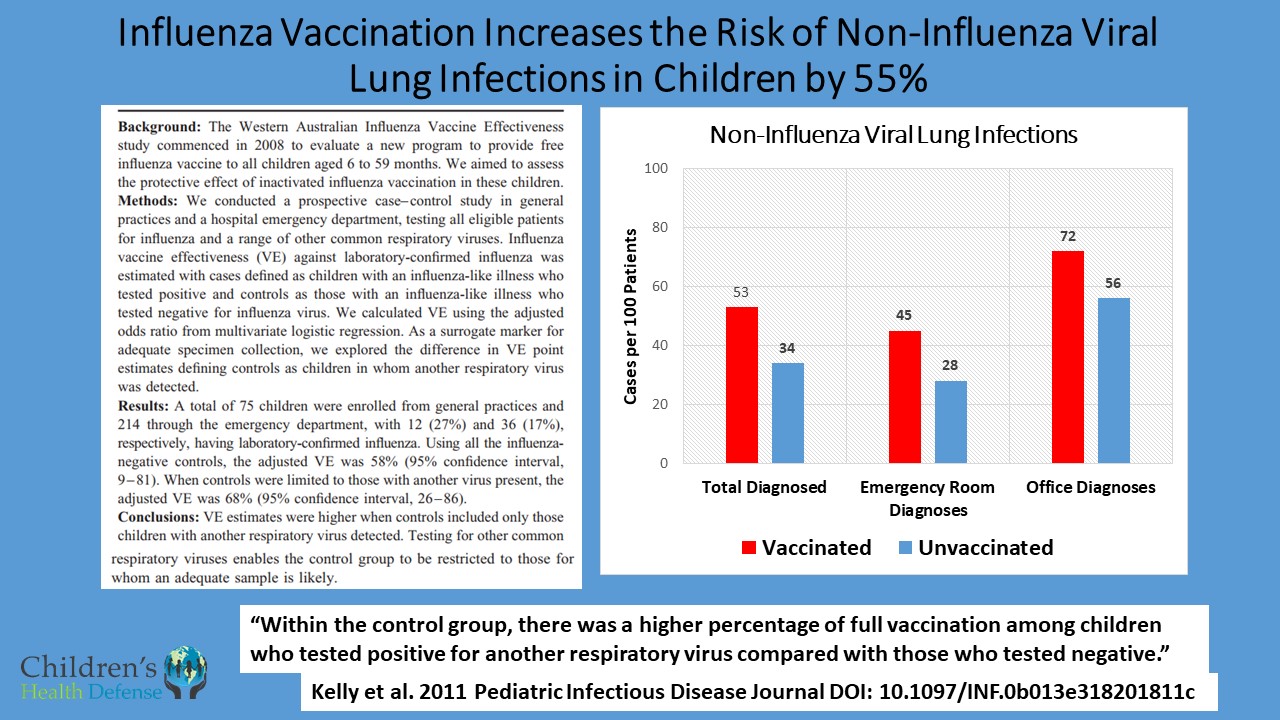
2011 Australian Study: Flu shot doubled risk of non-influenza viral infections and increased flu risk by 73%.
A prospective case-control study in healthy young Australian children found that seasonal flu shots doubled their risk of illness from non-influenza virus infections. Overall, the vaccine increased the risk of virus-associated acute respiratory illness, including influenza, by 73%.
https://childrenshealthdefense.org/news/vaccine-misinformation-flu-shots-equal-health/
Three New Studies Support Vitamin D’s Role in Preventing and Treating COVID-19
by Barbara Cáceres Published September 29, 2020 | Health, Holistic Health
Three new studies have reported the positive role of vitamin D in preventing COVID-19 and reducing the severity of illness in hospitalized patients with COVID-19 infection.
Researchers at Boston University conducted a retrospective, observational analysis1 of over 190,000 U.S. patients from 50 states with SARS-CoV-2 results performed mid-March through mid-June, 2020 and who had 25(OH)D (vitamin D) results from the preceding 12 months. Residential zip code data was matched with U.S. Census data to perform analyses of race/ethnicity proportions and latitude.
Vitamin D Deficiency Associated With 54 Percent Higher Risk for COVID-19
Those who had a circulating level of 25(OH)D below 20 ng/mL had a 54 percent higher positivity rate compared to those who had a blood level of 30–34 ng/mL. The risk of SARS-CoV-2 positivity continued to decline until the serum levels reached 55 ng/mL. The inverse relationship between SARS-CoV-2 positivity and 25(OH)D levels was most striking in predominately black non-Hispanic zip codes, followed by predominately Hispanic zip codes.
Calling the results “remarkable,” researcher Michael Holick, MD, PhD, summarized, “If you’re vitamin D deficient, you have a 54 percent higher risk of acquiring this infection compared to people who were vitamin D sufficient,” he said. “This was for all ages, for all ethnicities and for all latitudes in the United States in all 50 states. So whether you’re in California, Florida, or Alaska this still remained the same.”2
Vitamin D Supplementation Can Maintain Healthy Levels of Vitamin D
Approximately 42 percent of the US population is vitamin D deficient3 but 82 percent of blacks and 61 percent of Hispanics are deficient,4 and 60 percent of nursing home residents are deficient.5 Dr. Holick says that vitamin D insufficiency is very common in sunny states like California and Florida because of sunscreen use and the fact that people avoid the midday sun when UVB rays trigger a reaction in skin cells that makes vitamin D. He states that supplementation is a safe and effective way to maintain healthy levels of vitamin D, and that infants need 400-1000 units a day, children 600-1000 units a day, and teens and adults need 1500-2000 units a day, but “if you’re obese you need two to three times more.”6
Vitamin D Status Can Affect Risk of Mortality from COVID-19
A second study,7 also co-authored by Dr. Holick, is a cross sectional analysis of 235 hospitalized patients infected with COVID-19 that found those with sufficient vitamin D status had significantly better outcomes. Of patients over 40 years of age, 9.7 percent of patients who were vitamin D sufficient died compared to 20 percent who were vitamin D insufficient or deficient. Only 6.3 percent of the patients over 40 years died with a blood level of 25(OH)D of 40 ng/mL or higher. The data analyses also revealed that the severe decrease in infection was less prevalent in patients who had sufficient levels of vitamin D. The authors suggest that anti-inflammatory role of vitamin D helps modulate the immune response by reducing the risk for cytokine storm in response to this viral infection.
A pilot study conducted in Cordoba, Spain, and published in the Journal of Steroid Biochemistry and Molecular Biology found that the administration of high dose calcifediol (a main metabolite of Vitamin D endocrine system) significantly reduced the need for ICU treatment of patients requiring hospitalization due to proven COVID-19.8
The study evaluated 76 consecutive patients hospitalized with COVID-19 infection and randomly assigned two thirds of the patients to receive oral calcifediol in addition to standard care (per hospital protocol). One third of the patients received only standard care.
Of 50 patients treated with calcifediol, one required admission to the ICU (2 percent), while of 26 untreated patients, 13 required admission (50 percent). Of the patients treated with calcifediol, none died, and all were discharged without complications. The 13 patients not treated with calcifediol, who were not admitted to the ICU, were discharged. Of the 13 patients admitted to the ICU, two died and the remaining 11 were discharged.
The study authors suggested that activation of the vitamin D receptor (VDR) signaling pathway may generate beneficial effects in acute respiratory distress syndrome (ARDS) by decreasing the cytokine/chemokine storm; regulating the renin‑angiotensin system; modulating neutrophil activity and by maintaining the integrity of the pulmonary epithelial barrier; stimulating epithelial repair, and tapering down increased coagulability of the blood.
Read more here: https://thevaccinereaction.org/2020/09/three-new-studies-support-vitamin-ds-role-in-preventing-and-treating-covid-19/
Bad Medicine
by Maureen McDonnel | Sep 25, 2020 | COVID-19, Uncategorized
Millions Against Medical Mandates’ Collaborative Communication Committee (comprised of over 30 people from different organizations within our movement) has been generating “packaged messages” in an attempt to reach and influence those unaware of fact-based science regarding vaccine safety and effectiveness. Here is our next message about “bad medicine,” including influenza vaccines. We are asking everyone to review the message below, extract what is relevant for your specific audience, or use the message in its entirety and send it out to your members, family, friends, followers, etc. Please help us push these messages out so more people can wake up to the deeper issues and rise up in solidarity against oppressive and unhealthy directives.
BAD MEDICINE
What is bad medicine? It is both the use of medical interventions that cause more harm than good as well as the failure to use helpful interventions. Moreover, “bad medicine” is the failure to personalize medicine to an individual patient’s needs. With the SARS-CoV-2/COVID-19 crisis that has put our nation – and much of the world – on an unending lockdown, medicine has run amuck.
Why, more than six months into this situation is Anthony Fauci just now mentioning the value of Vitamins C and D, both of which are highly protective for contracting viruses. Why wasn’t he loudly and regularly encouraging every American to protect and boost their immune systems with these widely available inexpensive (hello sunshine and Vitamin D!) vitamins from the very beginning?
Read on to learn more about bad medicine:
- Misuse and overuse of ventilators for COVID-19 patients
- SARS-CoV-2 vaccine trials
- Failure to use effective (and often inexpensive) treatments
- And maybe the biggest “bad medicine” debacle out there – the flu vaccine!
1. Over-Use of Ventilators for COVID-19 Patients was Bad Medicine
Early reports of large percentages of patients dying when placed on ventilators were deeply concerning. Doctors since have learned that not all COVID-19 patients need ventilation, that they were ventilating too many patients, and too soon. Where was the precautionary principle among the panic? https://bit.ly/363aDM3; https://wapo.st/3kJa2TY
2. SARS-CoV-2 Vaccine Trials are Bad Medicine
Many pages could be devoted to issues in the SARS-CoV-2 vaccine trials. Vaccine development is indeed proceeding at warp speed but we need to ask, at what cost? We now have a serious neurological injury –including at least one case and possibly two cases transverse myelitis – in the Oxford/Astra Zeneca trials: https://nyti.ms/2FXcjMB and other significant injuries in the early Moderna trials: https://bit.ly/307MAYB We must demand greater transparency on all injuries to fully understand vaccine risks The most compelling questions are the long and short term potential harms signaled from the clinical trials.
- What impact will messenger RNA (mRNA), used in several vaccine candidates, have on vaccinated people? Even very “pro” mRNA vaccine professionals recognize that there are risks associated with mRNA vaccines – none of which has yet made it to commercial production – including, in particular, the risk of autoimmune diseases (https://go.nature.com/2EzKpFQ) – despite no evidence the public will be screened for autoimmune risks before mass vaccination.
- What about the use of aborted fetal cell lines in the manufacture of several candidate vaccines: https://bit.ly/2G0JVZT? These male and female human DNA cells in various vaccines are being questioned as possible contributors to the exponential rise in gender dysphoria: https://bit.ly/3czcZUq
- What about the use of polyethylene glycol (PEG), a synthetic chemical to which over 70% of people are sensitive –a significant number sensitive to the point of risking anaphylaxis? Moderna has added this dangerous chemical to its vaccine and went so far as to warn its shareholders that the use of PEG was risky to the bottom-line but does not tell clinical trial participants of the risk to them and does not test participants for PEG sensitivity. https://bit.ly/3i2YlWt Not only does PEG carry safety risks, but it may also reduce vaccine efficacy!
- What about risk of antibody-dependent enhancement (or “pathogenic priming”), which creates a possibility that a vaccinated person later exposed to the disease develops far worse symptoms or even dies from a hyper-immune reaction? This risk was seen in animal trials for SARS vaccines years ago and in the recent scandal with Dengvaxia, a dengue fever vaccine, in the Philippines. https://bit.ly/33V6Q0N
- A silver lining here? The distrust surrounding the pharmaceutical industry and government has resulted in Pharma taking the unprecedented step of releasing several trial protocols but we must look at that carefully to determine if these trials were set up for “success” even if the vaccines are not actually safe or effective: https://wb.md/2S9F77f
3. Ignoring or Disparaging Good Medicine is Bad Medicine
The Alliance for Natural Health (ANH-USA) details in their article titled “COVID 411” many specific nutrients that are among the most noteworthy preventives for boosting our immune systems before we get sick. https://bit.ly/2QMBh3d. In particular, a number of therapies and medicines, particularly when combined with zinc, are promising:
- Hydroxychloroquine: https://bit.ly/2ChKtc3; https://bit.ly/3eBTmuf; https://bit.ly/3jbGxtW
- Ivermectin: https://bit.ly/3gSnnqS; https://bit.ly/3hU0GDM; https://bit.ly/32UOn45; https://bit.ly/2YXrWtE
- Quercetin: https://bit.ly/32PwhAh; https://bit.ly/2R1oDxr
- Hinokitiol: https://prn.to/2Z1MalY; https://bit.ly/34W501O
Additionally, there are many other natural treatments and oxidative therapies (using ozone or hydrogen peroxide, for example) that doctors such as David Brownstein, MD, are using with great success: https://bit.ly/34Xz9xA; https://bit.ly/3gQU6Ne. The MATH+ protocol from the Front Line Covid-19 Critical Care (FLCCC) Alliance for severely ill patients is also a good resource: https://bit.ly/3h0Hnrr; https://bit.ly/3bjgOfP.
4. Influenza and Flu Vaccines Shenanigans are Bad Medicine
Del Bigtree really nailed the coffin on flu vaccines on the September 24, 2020 episode of The High Wire, entitled, “Twindemic 2020?” Watch this episode for the most up to date information https://bit.ly/3i3iBqT – the flu issue is addressed beginning around minute 48.
The influenza vaccine’s risk/benefit ratio is high – vaccinating can cause very serious conditions, including neurological harm, autoimmune disease, and death. https://bit.ly/2RYS3wm We also know that getting a flu shot increases your risk of developing more serious non-flu respiratory infections (including some coronavirus infections). https://bit.ly/3ctdbo0 How do we justify the continued push for universal flu shots when the harm outweighs the good?
Yet, the pharmaceutical industry, with its allies in public health and at CDC, present flu as a major cause of death in the U.S., and push flu shots as if they have saved many lives. This information may help put things in perspective:
- Flu shots have caused more bad reactions than all other vaccines combined according to the Vaccine Adverse Events Reporting System (VAERS), and the Vaccine Injury Compensation Program. “Seven out of ten petitions filed between 2016 and 2017 to the NVICP were related to damages following influenza vaccine to adults or children…” https://bit.ly/2G4XFm8
- Flu shots only prevent actual influenza A or B infections, and their effectiveness varies from 10-60% and in most years recently are under 50% effective and often under 30% effective. https://bit.ly/2FRnypY; https://bit.ly/2G4XFm8
- The CDC reported that in the 2018-19 flu season: “Among adults hospitalized for the flu, the vaccine’s effectiveness against the H3N2 strain was reported at -43 percent.” This indicates that those who got their flu shot were more likely to be hospitalized for flu than those who did not get the vaccine! https://bit.ly/2FWKoMM
- A 2009 study by the American Thoracic Society found “…children who had received the flu vaccine [trivalent inactivated flu vaccine—TIV] had three times the risk of hospitalization, as compared to children who had not received the vaccine. In asthmatic children, there was a significantly higher risk of hospitalization [all emphasis mine] in subjects who received the TIV, as compared to those who did not…” This makes the emphasis for asthmatics to take flu shots particularly alarming. https://bit.ly/3ctdMpK
- Over 80% of influenza-like illness – what people generally call “the flu” – are NOT type A or B influenza. They are viral or bacterial flu-like illnesses that are not covered by influenza vaccines. https://bit.ly/2FRnypY
- According to the American Lung Association, flu-caused deaths, as recorded on death certificates over a 13-year period, range between a mere 257-1812 deaths per year in the entire U.S.! https://bit.ly/3652eYD (p.5).
- CDC lumps the pneumonia deaths together with flu deaths, but most pneumonia deaths are unrelated to influenza and therefore could not be prevented or lessened by a flu shot – even if they worked! https://bit.ly/3652eYD
- Universal flu shots violate science and common sense given their high risk to benefit ratio and fact that “Only about 3 percent of pneumonia and influenza deaths occurred in those under age 45.” https://bit.ly/3652eYD (p.6).
CALL TO ACTION:
- Contact FDA and demand transparency in all aspects of the SARS-CoV-2 clinical trials. 1-888-463-6332 Choose option 3 then 1
- Call your governor and state and federal legislators and challenge them on flu vaccine mandates.
- Call vaccine manufacturers and demand transparency.
Read more and take action here: https://mamm.org/bad-medicine/
August News
There is so much going on but the best thing I’ve seen all month is Plandemic Indoctornation. The virus is real, the pandemic is manufactured…this film has documented info… please watch and share! Mom

You can watch both the documentary and see an interview with the director here: https://thehighwire.com/videos/the-highwire-presents-plandemic-indoctornation-2/
Other links to the movie:
https://www.bitchute.com/video/4u7rt61YeGox/https://www.bitchute.com/video/4u7rt61YeGox/
July News
I find it very interesting that the ‘news’ and ‘public health’ sources make all these proclamations but never bother to cite scientific references. All of what they call ‘anti-vaccine’ sites include the links to the actual science.
Always follow the science and follow the money.
Mom
A great series of talks here. Both Dr’s are brilliant and share lots of interesting info. The link is to episode 4, but I do suggest starting at episode 1 and watching them all.
https://disseminate.tv/watch/critically-thinking-with-dr-t-and-dr-p-episode-4_TjkC5BntSkxfv3F.html
Great, brand new film about the 1986 Act that took away liability for vaccine manufacturers. Really important info to watch and share. http://1986theact.com/
The best weekly show I have found for accurate information about what is going on in these crazy times is The Highwire with Del Bigtree. Here’s this weeks show:
Another very interesting video from today, Attorneys Robert F Kennedy jr, and Alan Dershowizt did a vaccine debate this morning. We need to be able to talk about vaccines, vaccine injury and the tobacco science that the companies are using.
That’s this months new. Be well and stand strong. Mom
LOCKDOWN LUNACY: The Thinking Person’s Guide

Great article from the brilliant JB Handley and Children’s Health Defense.
By J.B. Handley, CHD Contributing Writer
For anyone willing to look, there are so many facts that tell the true story, and it goes something like this:
Knowing what we know today about COVID-19’s Infection Fatality Rate, asymmetric impact by age and medical condition, non-transmissibility by asymptomatic people and in outdoor settings, near-zero fatality rate for children, and the basic understanding of viruses through Farr’s law, locking down society was a bone-headed policy decision so devastating to society that historians may judge it as the all-time worst decision ever made. Worse, as these clear facts have become available, many policy-makers haven’t shifted their positions, despite the fact that every hour under any stage of lockdown has a domino-effect of devastation to society. Meanwhile, the media—with a few notable exceptions—is oddly silent on all the good news. Luckily, an unexpected group of heroes across the political landscape—many of them doctors and scientists—have emerged to tell the truth, despite facing extreme criticism and censorship from an angry mob desperate to continue fighting an imaginary war.
My goal is to engage in known facts. You, the reader, can decide if all of these facts, when you put them together, equate to the story above.
Fact #1: The Infection Fatality Rate for COVID-19 is somewhere between 0.07-0.20%, in line with seasonal flu
The Infection Fatality Rate math of ANY new virus ALWAYS declines over time as more data becomes available, as any virologist could tell you. In the early days of COVID-19 where we only had data from China, there was a fear that the IFR could be as high as 3.4%, which would indeed be cataclysmic. On April 17th, the first study was published from Stanford researchers that should have ended all lockdowns immediately, as the scientists reported that their research “implies that the infection is much more widespread than indicated by the number of confirmed cases” and pegged the IFR between 0.12-0.2%. The researchers also speculated that the final IFR, as more data emerged, would likely “be lower.” For context, seasonal flu has an IFR of 0.1%. Smallpox? 30%.
As the first study to peg the IFR, the Stanford study came under withering criticism, prompting the lead researcher, Dr. John Ioannidis to note,
“There’s some sort of mob mentality here operating that they just insist that this has to be the end of the world, and it has to be that the sky is falling. It’s attacking studies with data based on speculation and science fiction. But dismissing real data in favor of mathematical speculation is mind-boggling.”
Like all good science, the Stanford data on IFR has now been replicated so many times that our own Centers for Disease Control came out this week to announce that their ‘best estimate’ showed an IFR below 0.3%. In this article on the CDC’s new data, they also highlighted how the cascading declines in IFR has removed all the fears of doomsday:
That “best estimate” scenario also assumes that 35 percent of infections are asymptomatic, meaning the total number of infections is more than 50 percent larger than the number of symptomatic cases. It therefore implies that the IFR is between 0.2 percent and 0.3 percent. By contrast, the projections that the CDC made in March, which predicted that as many as 1.7 million Americans could die from COVID-19 without intervention, assumed an IFR of 0.8 percent. Around the same time, researchers at Imperial College produced a worst-case scenario in which 2.2 million Americans died, based on an IFR of 0.9 percent.
If you’re still unconvinced that the IFR of COVID-19 is roughly in line with a bad flu season, the most comprehensive analysis I have seen comes from Oxford University, who recently stated:
“Taking account of historical experience, trends in the data, increased number of infections in the population at largest, and potential impact of misclassification of deaths gives a presumed estimate for the COVID-19 IFR somewhere between 0.1% and 0.41%.”
Finally, just last week, Stanford’s Dr. Ioannidis published a meta-analysis (because so many IFR studies have been done around the world in April and early May) where he analyzed TWELVE separate IFR studies and his conclusion is so good, I’ll just leave you with it:
The infection fatality rate (IFR), the probability of dying for a person who is infected, is one of the most critical and most contested features of the coronavirus disease 2019 (COVID-19) pandemic. The expected total mortality burden of COVID-19 is directly related to the IFR. Moreover, justification for various non-pharmacological public health interventions depends crucially on the IFR. Some aggressive interventions that potentially induce also more pronounced collateral harms1 may be considered appropriate, if IFR is high. Conversely, the same measures may fall short of acceptable risk-benefit thresholds, if the IFR is low…Interestingly, despite their differences in design, execution, and analysis, most studies provide IFR point estimates that are within a relatively narrow range. Seven of the 12 inferred IFRs are in the range 0.07 to 0.20 (corrected IFR of 0.06 to 0.16) which are similar to IFR values of seasonal influenza. Three values are modestly higher (corrected IFR of 0.25-0.40 in Gangelt, Geneva, and Wuhan) and two are modestly lower than this range (corrected IFR of 0.02-0.03 in Kobe and Oise).
Opinion #1: Dr. Scott Atlas
Soon after the Stanford study released its data (he wasn’t a study author), Stanford’s Dr. Scott Atlas published an opinion piece in The Hill newspaper with the title, “The data is in — stop the panic and end the total isolation.” He wrote:
The recent Stanford University antibody study now estimates that the fatality rate if infected is likely 0.1 to 0.2 percent, a risk far lower than previous World Health Organization estimates that were 20 to 30 times higher and that motivated isolation policies…Let’s stop underemphasizing empirical evidence while instead doubling down on hypothetical models. Facts matter.
Facts do matter, but no one listened. Dr. Atlas’ article also helps frame Fact #2.
Fact #2: The risk of dying from COVID-19 is much higher than the average IFR for older people and those with co-morbidities, and much lower than the average IFR for younger healthy people, and nearing zero for children
In January 2020, Los Angeles had an influenza outbreak that was killing children, the LA Times noted that “an unlikely strain of influenza has sickened and killed an unusually high number of young people in California this flu season.” COVID-19 is the opposite of that. Stanford’s Dr. Ioannidis said, “Compared to almost any other cause of disease that I can think of, it’s really sparing young people.”
Italy reported three days ago that 96% of Italians who died from COVID-19 had “other illnesses” and were, on average, 80 years old. From Bloomberg:
“The latest numbers show that new cases and fatalities have a common profile: mostly elderly people with previous illnesses,” ISS chief Silvio Brusaferro said at a news conference Friday.
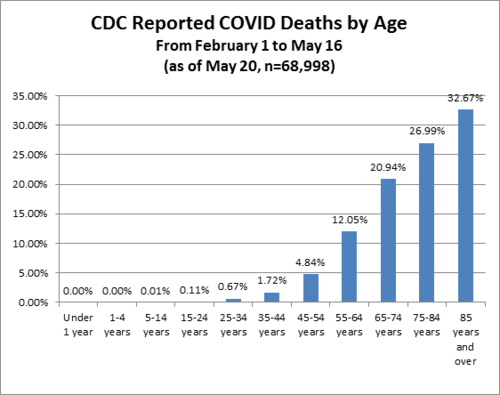
The best age stratification data I have seen comes from Worldometers.info. Here’s their chart estimating death rate by age group. Please note that death rate is MUCH higher than IFR because death rate uses confirmed COVID-19 cases as the denominator, but it shows you how different the fatality rates are by age:
While this data is “crude”, it’s safe to extrapolate that an 80+ year-old person has a serious risk of dying from COVID-19 while a child faces almost no risk. This fact should drive policy, as Dr. Atlas explains:
Of all fatal cases in New York state, two-thirds were in patients over 70 years of age; more than 95 percent were over 50 years of age; and about 90 percent of all fatal cases had an underlying illness. Of 6,570 confirmed COVID-19 deaths fully investigated for underlying conditions to date, 6,520, or 99.2 percent, had an underlying illness. If you do not already have an underlying chronic condition, your chances of dying are small, regardless of age. And young adults and children in normal health have almost no risk of any serious illness from COVID-19.
Consider this excellent article from the British Medical Journal, titled “Shielding from covid-19 should be stratified by risk” written by Cambridge University professors:
Protecting those at most risk of dying from covid-19 while relaxing the strictures on others provides a way forward in the SARS-CoV-2 epidemic, given the virus is unlikely to disappear in the foreseeable future. Such targeted approaches would, however, require a shift away from the notion that we are all seriously threatened by the disease, which has led to levels of personal fear being strikingly mismatched to objective risk of death. Instead, the aim should be to communicate realistic levels of risk as they apply to different groups, not to reassure or frighten but to allow informed personal decisions in a setting of necessary uncertainty.
As one simple example: closing schools makes almost no sense given what we know about COVID-19, while protecting teachers over the age of 60—to pick a somewhat defensible age boundary—may well make sense. This is why so many countries who seem to respect data more than we do here in the U.S. have already re-opened their schools. In fact, Denmark’s schools have been open since mid-April!! And, for those keeping score, Reuters just reported yesterday that, “Reopening schools in Denmark did not worsen outbreak, data shows.” Here’s a quote:
“You cannot see any negative effects from the reopening of schools,” Peter Andersen, doctor of infectious disease epidemiology and prevention at the Danish Serum Institute said on Thursday told Reuters. In Finland, a top official announced similar findings on Wednesday, saying nothing so far suggested the coronavirus had spread faster since schools reopened in mid-May.
Another great article on schools, titled, “It is fear – not science – that is stopping our children being educated” in The Telegraph newspaper last week, here’s a quote:
There is little about coronavirus we can be absolutely sure of – this is a brand new disease and our knowledge grows by the day – but most of the available evidence so far strongly suggests that children are neither suffering from coronavirus nor spreading it. Studies in South Korea, Iceland, Italy, Japan, France, China, the Netherlands and Australia all concur that youngsters are “not implicated significantly in transmitting Covid”, not even to parents and siblings.
Adult paranoia, stoked by over-the-top government messaging, union intransigence and media conniptions, is now being inflicted on the youngest members of our society to whom the virus poses a threat so tiny scientists call it “statistically irrelevant”. Instead of nursery rhymes, mixed infants may soon be invited to sing something called the “two-metre-song” as they stick their arms out to keep their friends at bay.
Brand new science (May 28) released from Northern Ireland clearly shows that schoolchildren do NOT serve as vectors for COVID-19. Titled, No evidence of secondary transmission of COVID-19 from children attending school in Ireland, 2020, the study could not be more clear:
These findings suggest that schools are not a high risk setting for transmission of COVID-19 between pupils or between staff and pupils. Given the burden of closure outlined by Bayhem [4] and Van Lanker [5], reopening of schools should be considered as an early rather than a late measure in the lifting of restriction.
Finally, Dr. Scott Atlas took on the topic of schools in this recent interview:
“There’s no science whatsoever to keep K-through-12 schools closed, nor to have masks or social distancing on children, nor to keep summer programs closed. What we know now is that the risk of death and the risk of even a serious illness is nearly zero in people under 18.
Quick update: after I wrote this, the Wall Street Journal published this article titled Is It Safe to Reopen Schools? These Countries Say Yes. To me, this reads as a bit of a litmus test for countries that have independent and data-driven public health officials, and I give the U.S. an ‘F” for our current approach:
But Denmark, Austria, Norway, Finland, Singapore, Australia, New Zealand and most other countries that have reopened classrooms haven’t had outbreaks in schools or day-care centers…In Denmark, the opening of schools had no impact on the progress of the epidemic, said Tyra Grove Krause, a senior official with the State Serum Institute, the country’s disease control agency…Since Austria reopened on May 18, no increase in infections has been observed in schools and kindergartens, a spokesman for the government said…In Norway, the government won’t close schools again even if the number of cases starts rising in the country because there have been no negative consequences from reopening schools on April 20, said Education Minister Guri Melby.
How many more countries need to re-open before the U.S. follows? Seriously, it’s a little embarrassing to be American…IMO we look like total chumps.
Update #2: Dr. Scott Atlas doubled-down on June 1st with this great Op-Ed, once again in The Hill, titled Science says: ‘Open the schools’. As usual, he’s amazingly eloquent, here’s an excerpt but well worth the time to read every word, he simply slays it:
All of this borders on the absurd, when we now know that social distancing and face coverings for children are completely unnecessary.
Never have schools subjected children to such an unhealthy, uncomfortable and anti-educational environment, so science cannot precisely define the total harm it will cause. But science does tell us that risks from COVID-19 are too minimal to sacrifice the educational, social, emotional and physical well-being – to say nothing of the very health – of our young people.
(Special note: there’s a new boogeyman, Kawasaki disease, that some are trying to link to COVID-19. Here’s a great article about that, or see the website of the UK’s Kawasaki Disease Foundation where they discuss the “mishandling of information” about Kawasaki disease. Dr. Atlas’ most recent post discusses this, too: “What about the new threat similar to Kawasaki disease, recently sensationalized as a COVID-19 association? In fact, the association is extremely low, and the incidence of the disorder is itself rare, affecting only 3,000 to 5,000 children in the United States each year. Importantly, the syndrome is typically treatable and never has been regarded previously as a risk so serious that schools must be shuttered.”)
Fact #3: People infected with COVID-19 who are asymptomatic (which is most people) do NOT spread COVID-19

On January 13, 2020, a 22-year old female with a history of congenital heart disease went to the emergency room of Guangdong Provincial People’s Hospital complaining of a variety of symptoms common to people with her condition, including pulmonary hypertension and shortness of breath due to atrial septal defect (hole in the heart). Little did she know her case would set off a cascade of events resulting in a recently published paper that should have ended all lockdowns around the world simultaneously. Three days into her hospital stay, her condition was improving. Routine tests were run, and to the clinicians alarm and surprise, she tested positive for COVID-19. As the physicians noted, “the patient had never fever, sore throat, myalgia or other symptoms associated with virus infection.” Said differently, she was completely asymptomatic for COVID-19.
It’s not that easy to find people who are infected with COVID-19 but asymptomatic, because they don’t seek medical attention. Here in Oregon where I live, you can’t even get a COVID-19 test unless you have symptoms. So, the stars aligned to put this woman in a hospital with researchers studying COVID-19, and she became the subject of an extensive contact study published on May 13 in Respiratory Medicine, titled, “A study on infectivity of asymptomatic SARS-CoV-2 carriers.”
The researchers wanted to find out whether this woman, with a COVID-19 infection but no symptoms, had infected anyone else, so they chose to look at every single contact they could identify within the previous 5 days prior to her positive test. So, how many people did they have to screen? 455. Not a small number, as the researchers explain:
455 contacts who were exposed to the asymptomatic COVID-19 virus carrier became the subjects of our research. They were divided into three groups: 35 patients, 196 family members and 224 hospital staffs. We extracted their epidemiological information, clinical records, auxiliary examination results and therapeutic schedules.
As you can see, being hospitalized led to the majority of the contacts this woman had, both with other patients and with many members of the hospital staff. Notably, all of these contacts took place indoors and one might argue many of the contacts—at least with hospital staff—would have involved relatively intimate contact. Amongst the patients, the average age was 62, arguably making them higher risk, and many of those patients were immunocompromised for a variety of reasons, including chemotherapy and cardiovascular disease. So how many of the 455 people were infected by the asymptomatic 22-year old woman?
“In summary, all the 455 contacts were excluded from SARS-CoV-2 infection…”
Said differently, exactly zero people were infected. The scientists, in typically understated fashion, offer up a comment about the question I hope you are asking yourself right now (namely, why are we all on lockdown if asymptomatic people with COVID-19 can’t spread the infection?), stating, “the result of this study may alleviate parts of the public concern about asymptomatic infected people.”
If this study had been published in early March, the odds that the world would have locked down are very, very low. Yet, this study, published only two weeks ago, is nowhere to be found in the media, and is never mentioned by policy makers. It just sits there, sharing the truth for anyone willing to listen.
Fact #4: Emerging science shows no spread of COVID-19 in the community (shopping, restaurants, barbers, etc.)
“There is no significant risk of catching the disease when you go shopping. Severe outbreaks of the infection were always a result of people being closer together over a longer period of time…”
– Professor Hendrick Streek , University of Bonn
We just learned that asymptomatic people infected with COVID-19 are very unlikely to be able to spread the infection to others. Emerging and published science shows transmission of COVID-19 in retail establishments is extremely unlikely. Professor Hendrik Streeck from the University of Bonn is leading a study in Germany on the hard-hit region of Heinsberg and his conclusions, from laboratory work already completed, is very clear:

“There is no significant risk of catching the disease when you go shopping. Severe outbreaks of the infection were always a result of people being closer together over a longer period of time.
“When we took samples from door handles, phones or toilets it has not been possible to cultivate the virus in the laboratory on the basis of these swabs….”
Uh oh. You mean closing parks, closing stores, wearing gloves and masks at the grocery store, fumigating our groceries, and just being generally paranoid wasn’t necessary? As Dr. Streeck confirms:
“It is important to obtain this data in order to make sure that decisions are taken based on facts rather than assumptions. The data should serve as a basis of information for the government so they can then think about their further course of action,” he said.
And he continues:
“People could lose their jobs. They might not be able to pay their rent anymore and staying inside for a longer time can lead to weakening of our immune system.”
“The goal is not a complete containment of the virus. We need to know where the actual capacity limits of our hospitals are. How many infections are too many? What do intensive care medics say?”
And, finally:
“It is important to start thinking about a ‘rollback’ strategy and his hope is to “deliver the relevant facts so that people have a good foundation for their decisions.”
Fact #5: Published science shows COVID-19 is NOT spread outdoors

In a study titled Indoor transmission of SARS-CoV-2 and published on April 2, 2020, scientists studied outbreaks of 3 or more people in 320 separate towns in China over a five-week period beginning in January 2020 trying to determine WHERE outbreaks started: in the home, workplace, outside, etc.? What’d they discover? Almost 80% of outbreaks happened in the home environment. The rest happened in crowded buses and trains. But what about outdoors? The scientists wrote:
“All identified outbreaks of three or more cases occurred in an indoor environment, which confirms that sharing indoor space is a major SARS-CoV-2 infection risk.”
Said differently, there’s really no science to support all the outdoor bans that my home state of Oregon and so many other states have put in place. I’ll leave you with my favorite quote from the study because it’s really quite infuriating to read when you consider some of the ways Governors here in the U.S have behaved (and some still do) by banning all sorts of outdoor activities, arresting paddle boarders on the water, etc.:
“The transmission of respiratory infections such as SARS-CoV-2 from the infected to the susceptible is an indoor phenomenon.”
Quick Update: Apparently the health minister of British Columbia, Canada, got the memo about the lack of airborne risk, this article appeared on June 1:

One of B.C.’s top health officials, however, says medical professionals have a pretty clear picture of how the virus is transmitted. “There is absolutely no evidence that this disease is airborne, and we know that if it were airborne, then the measures that we took to control COVID-19 would not have worked,” Dr. Reka Gustafson, B.C.’s deputy provincial health officer, told CTV Morning Live Monday.”We are very confident that the majority of transmission of this virus is through the droplet and contact route….”The overwhelming majority of (COVID-19) transmissions occur through close, prolonged contact and that is not the pattern of transmission we see through airborne diseases,” she said.
I sure hope Major League Baseball, the National Football League, and the NCAA are all paying attention…not to mention all the people in Portland here still riding bikes and running with masks on.
Fact #6: Science shows masks are ineffective to halt the spread of COVID-19, and The WHO recommends they should only be worn by healthy people if treating or living with someone with a COVID-19 infection
May 29th, the World Health Organization announced that masks should only be worn by healthy people if they are taking care of someone infected with COVID-19:
“If you do not have any respiratory symptoms such as fever, cough or runny nose, you do not need to wear a mask,” Dr. April Baller, a public health specialist for the WHO, says in a video on the world health body’s website posted in March. “Masks should only be used by healthcare workers, caretakers or by people who are sick with symptoms of fever and cough.”
Just before the COVID-19 madness, researchers in Hong Kong submitted a study for publication with the mouthful of a title, “Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings—Personal Protective and Environmental Measures.” Oddly, the study, just published this month, is actually housed on the CDC’s own website, and directly contradicts recent advice from the CDC about wearing a mask. Namely, the study states:
“In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018….In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks…Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza….Proper use of face masks is essential because improper use might increase the risk for transmission.”
English translation: there is no evidence that wearing masks reduces the transmission of respiratory illnesses and, if masks are worn improperly (like when people re-use cloth masks), transmission could actually INCREASE. Moreover, this study was a meta-analysis, which means it dug deep into the archive of science (all the way back to 1946!) to reach its conclusions. Said differently, this is as comprehensive as science gets, and their conclusions were crystal clear: masks for the general population show no evidence of working to either slow the spread of respiratory viruses or protect people.
This study is far from the only one to reach this conclusion (which makes the choice of a grocery store chain like my beloved New Seasons to make masks mandatory for all customers really quite unbelievable). The purpose of science is to arbitrate these thorny issues and while the science is clear, the hysteria continues. It turns out, the effectiveness of masks has a long history of debate in the medical community, which explains why so much science has been done on the topic. I will just highlight a few studies before you fall asleep:
My favorite article is actually a review of much of the science and it’s a great place to start for anyone who likes to do their own research. Titled, “Why Face Masks Don’t Work: A Revealing Review”, it was written to challenge the need for dentists to wear face masks, but all the science quoted and conclusions drawn apply to airborne pathogens in any setting. Some of the best quotes:
“The science regarding the aerosol transmission of infectious diseases has, for years, been based on what is now appreciated to be ‘very outmoded research and an overly simplistic interpretation of the data.’ Modern studies are employing sensitive instruments and interpretative techniques to better understand the size and distribution of potentially infectious aerosol particles…The primary reason for mandating the wearing of face masks is to protect dental personnel from airborne pathogens. This review has established that face masks are incapable of providing such a level of protection.”
And my favorite quote:
“It should be concluded from these and similar studies that the filter material of face masks does not retain or filter out viruses or other submicron particles. When this understanding is combined with the poor fit of masks, it is readily appreciated that neither the filter performance nor the facial fit characteristics of face masks qualify them as being devices which protect against respiratory infections. ”
Here’s an article published in ResearchGate by noted Canadian physicist D.G. Rancourt, written directly in response to the COVID-19 outbreak, published last month. Titled, Masks Don’t Work: A review of science relevant to COVID-19 social policy.
“Masks and respirators do not work. There have been extensive randomized controlled trial (RCT) studies, and meta-analysis reviews of RCT studies, which all show that masks and respirators do not work to prevent respiratory influenza-like illnesses, or respiratory illnesses believed to be transmitted by droplets and aerosol particles. Furthermore, the relevant known physics and biology, which I review, are such that masks and respirators should not work. It would be a paradox if masks and respirators worked, given what we know about viral respiratory diseases: The main transmission path is long-residence-time aerosol particles (< 2.5 μm), which are too fine to be blocked, and the minimum-infective-dose is smaller than one aerosol particle.”
To put this in simple terms: in order for a mask to really be effective that covered both your nose and mouth, you would asphyxiate. The minute the mask allows you to breathe, it can no longer filter the micro-particles that make you sick.
Finally, I often see this study from 2015 in the BMJ cited: “A cluster randomised trial of cloth masks compared with medical masks in healthcare workers“, and it bears repeating, since MOST of the masks I see people wearing in the community right now are cloth masks. Not only are these masks 100% ineffective at reducing the spread of COVID-19, but they can actually harm you. As the researchers explain:
“This study is the first RCT of cloth masks, and the results caution against the use of cloth masks. This is an important finding to inform occupational health and safety. Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection. Further research is needed to inform the widespread use of cloth masks globally.”
Increased risk of infection? Yes, that’s what it says. Other studies have also looked at the impact masks have on your oxygen levels (because you’re are forced to re-breathe your own Co2) and it’s not good. Scientists looked at oxygen levels of surgeons wearing masks while performing surgery and found: “Our study revealed a decrease in the oxygen saturation of arterial pulsations (SpO2) and a slight increase in pulse rates compared to preoperative values in all surgeon groups.”
Just this past week, this article came out in the New England Journal of Medicine, written my several doctors and public health officials with the title, “Universal Masking in Hospitals in the Covid-19 Era,” and this statement seems a perfect way to end my discussion of masks:
We know that wearing a mask outside health care facilities offers little, if any, protection from infection. Public health authorities define a significant exposure to Covid-19 as face-to-face contact within 6 feet with a patient with symptomatic Covid-19 that is sustained for at least a few minutes (and some say more than 10 minutes or even 30 minutes). The chance of catching Covid-19 from a passing interaction in a public space is therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic.
Read the rest here: https://childrenshealthdefense.org/news/lockdown-lunacy-the-thinking-persons-guide/