September News
Here’s the best of the recent news. Love, Mom
Pentagon Study: Flu Shot Raises Risk of Coronavirus by 36% (and Other Supporting Studies)
By Robert F. Kennedy, Jr., Chairman, Children’s Health Defense
On March 12th, 2020, Anderson Cooper and Dr. Sanjay Gupta held a global town hall on “Corona Facts and Fears.” During the discussion, Anderson said to the viewing audience, “And, again, if you are concerned about coronavirus, and you haven’t gotten a flu shot…you should get a flu shot.”
Setting safety and efficacy of influenza vaccination aside, is Anderson’s claim that the flu shot will help people fight COVID-19 remotely true? The short answer is no.
In fact, the results of many peer-reviewed, published studies prove that Anderson’s recommendation may have been the worst advice he could have given the public.
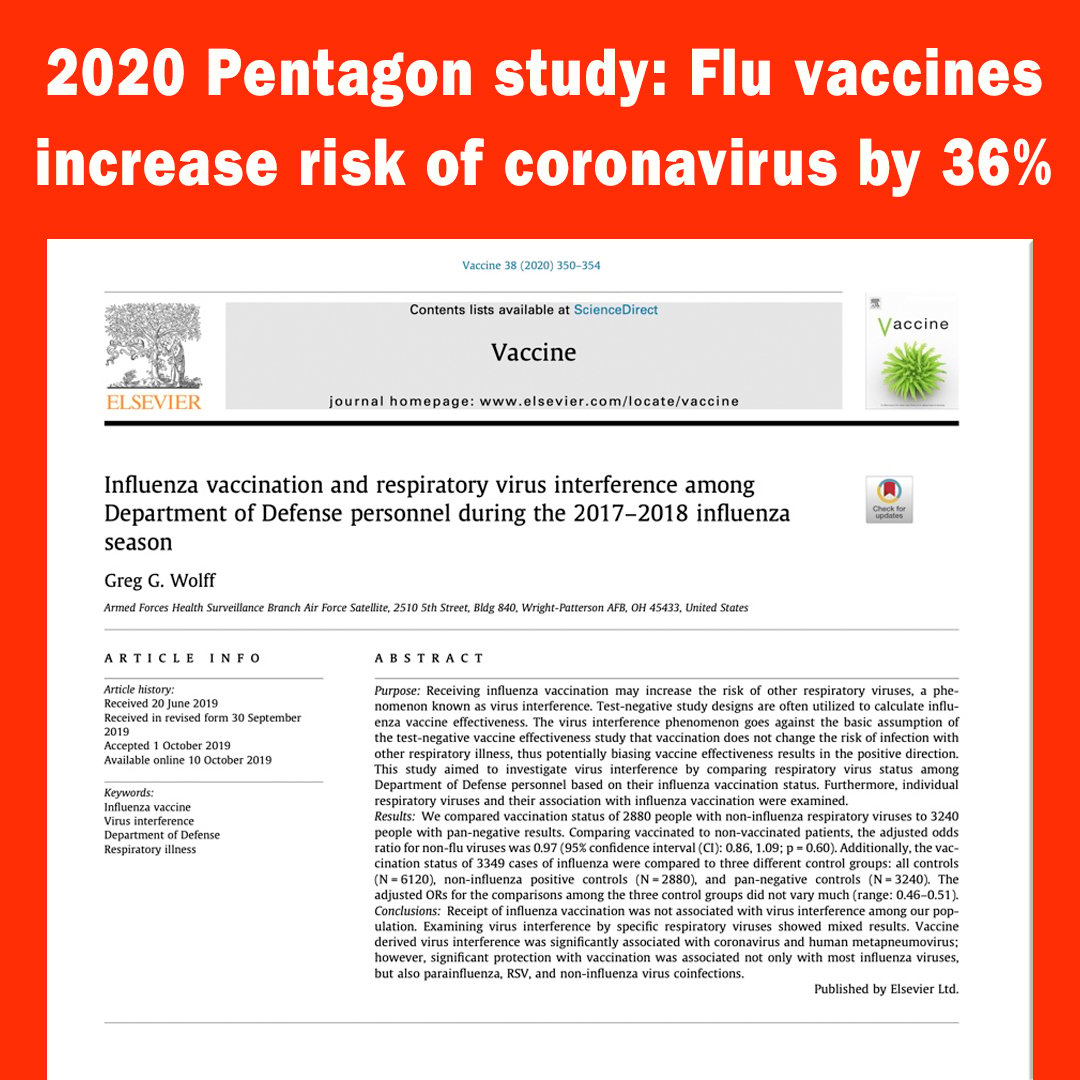
In searching the literature, the only study we have been able to find assessing flu shots and coronavirus is a 2020 US Pentagon study that found that the flu shot INCREASES the risks from coronavirus by 36%. “Receiving influenza vaccination may increase the risk of other respiratory viruses, a phenomenon known as “virus interference…’vaccine derived’ virus interference was significantly associated with coronavirus…” Here are the findings:
2020 Pentagon study: Flu vaccines increase risk of coronavirus by 36%
Examining non-influenza viruses specifically, the odds of coronavirus in vaccinated individuals were significantly higher when compared to unvaccinated individuals with an odds ratio (association between an exposure and an outcome) of 1.36. In other words, the vaccinated were 36% more likely to get coronavirus.

Many other studies suggest the increased risk of viral respiratory infections from the flu shot:
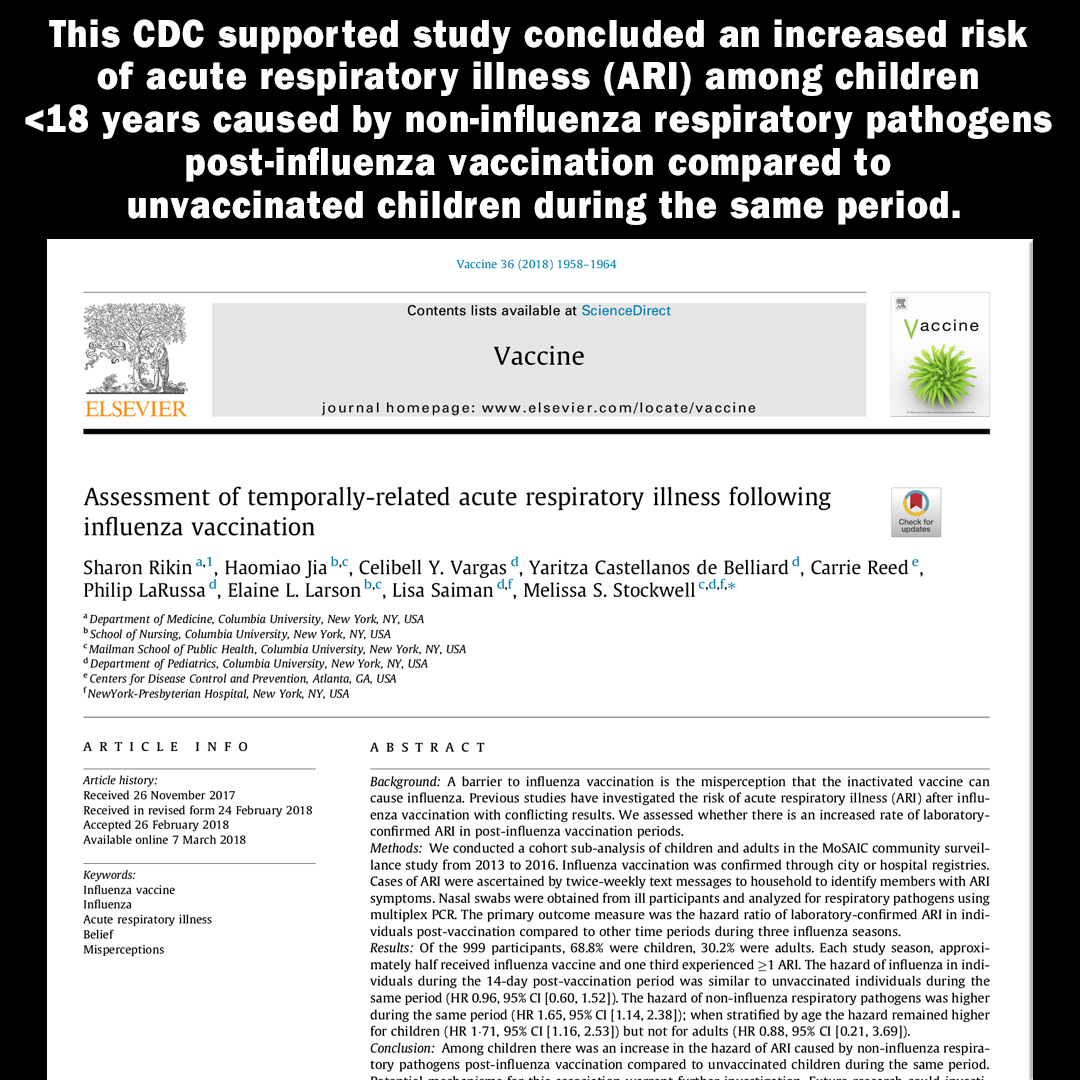
2018 CDC Study: Flu shots increase risk of non-flu acute respiratory illnesses (ARI) in children.
This CDC supported study concluded an increased risk of acute respiratory illness (ARI) among children <18 years caused by non-influenza respiratory pathogens post-influenza vaccination compared to unvaccinated children during the same period.

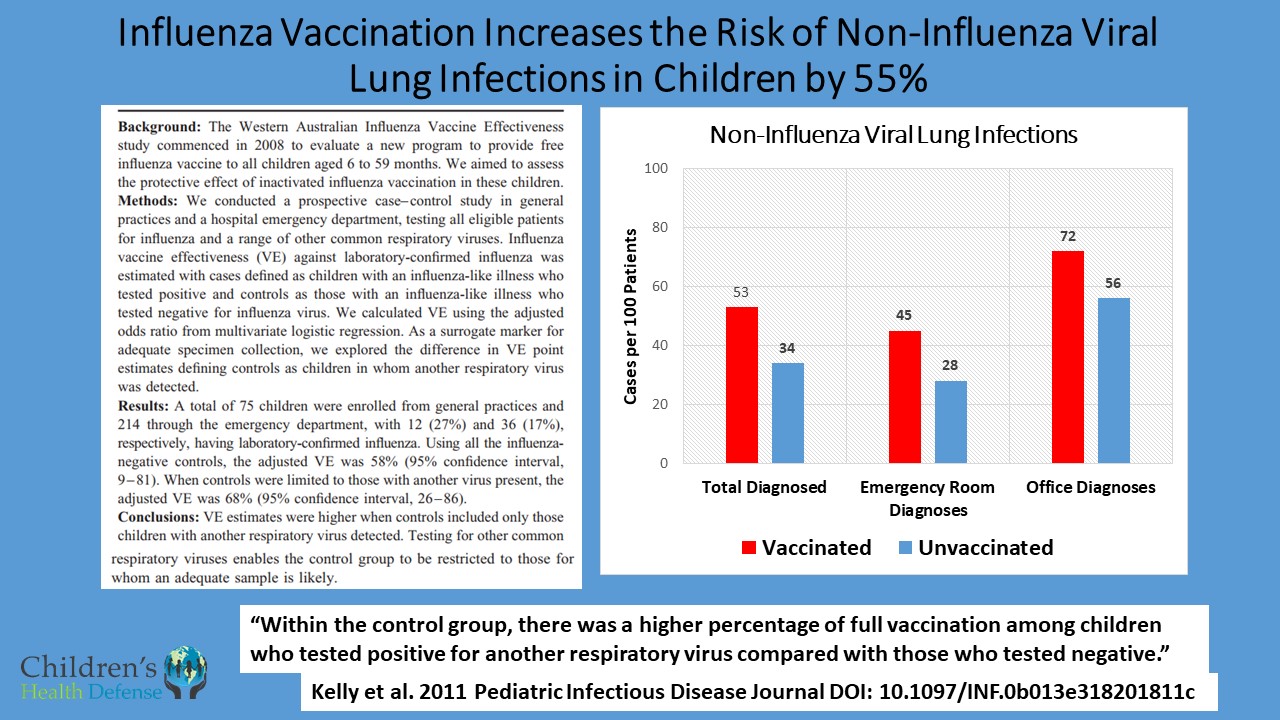
2011 Australian Study: Flu shot doubled risk of non-influenza viral infections and increased flu risk by 73%.
A prospective case-control study in healthy young Australian children found that seasonal flu shots doubled their risk of illness from non-influenza virus infections. Overall, the vaccine increased the risk of virus-associated acute respiratory illness, including influenza, by 73%.
https://childrenshealthdefense.org/news/vaccine-misinformation-flu-shots-equal-health/
Three New Studies Support Vitamin D’s Role in Preventing and Treating COVID-19
by Barbara Cáceres Published September 29, 2020 | Health, Holistic Health
Three new studies have reported the positive role of vitamin D in preventing COVID-19 and reducing the severity of illness in hospitalized patients with COVID-19 infection.
Researchers at Boston University conducted a retrospective, observational analysis1 of over 190,000 U.S. patients from 50 states with SARS-CoV-2 results performed mid-March through mid-June, 2020 and who had 25(OH)D (vitamin D) results from the preceding 12 months. Residential zip code data was matched with U.S. Census data to perform analyses of race/ethnicity proportions and latitude.
Vitamin D Deficiency Associated With 54 Percent Higher Risk for COVID-19
Those who had a circulating level of 25(OH)D below 20 ng/mL had a 54 percent higher positivity rate compared to those who had a blood level of 30–34 ng/mL. The risk of SARS-CoV-2 positivity continued to decline until the serum levels reached 55 ng/mL. The inverse relationship between SARS-CoV-2 positivity and 25(OH)D levels was most striking in predominately black non-Hispanic zip codes, followed by predominately Hispanic zip codes.
Calling the results “remarkable,” researcher Michael Holick, MD, PhD, summarized, “If you’re vitamin D deficient, you have a 54 percent higher risk of acquiring this infection compared to people who were vitamin D sufficient,” he said. “This was for all ages, for all ethnicities and for all latitudes in the United States in all 50 states. So whether you’re in California, Florida, or Alaska this still remained the same.”2
Vitamin D Supplementation Can Maintain Healthy Levels of Vitamin D
Approximately 42 percent of the US population is vitamin D deficient3 but 82 percent of blacks and 61 percent of Hispanics are deficient,4 and 60 percent of nursing home residents are deficient.5 Dr. Holick says that vitamin D insufficiency is very common in sunny states like California and Florida because of sunscreen use and the fact that people avoid the midday sun when UVB rays trigger a reaction in skin cells that makes vitamin D. He states that supplementation is a safe and effective way to maintain healthy levels of vitamin D, and that infants need 400-1000 units a day, children 600-1000 units a day, and teens and adults need 1500-2000 units a day, but “if you’re obese you need two to three times more.”6
Vitamin D Status Can Affect Risk of Mortality from COVID-19
A second study,7 also co-authored by Dr. Holick, is a cross sectional analysis of 235 hospitalized patients infected with COVID-19 that found those with sufficient vitamin D status had significantly better outcomes. Of patients over 40 years of age, 9.7 percent of patients who were vitamin D sufficient died compared to 20 percent who were vitamin D insufficient or deficient. Only 6.3 percent of the patients over 40 years died with a blood level of 25(OH)D of 40 ng/mL or higher. The data analyses also revealed that the severe decrease in infection was less prevalent in patients who had sufficient levels of vitamin D. The authors suggest that anti-inflammatory role of vitamin D helps modulate the immune response by reducing the risk for cytokine storm in response to this viral infection.
A pilot study conducted in Cordoba, Spain, and published in the Journal of Steroid Biochemistry and Molecular Biology found that the administration of high dose calcifediol (a main metabolite of Vitamin D endocrine system) significantly reduced the need for ICU treatment of patients requiring hospitalization due to proven COVID-19.8
The study evaluated 76 consecutive patients hospitalized with COVID-19 infection and randomly assigned two thirds of the patients to receive oral calcifediol in addition to standard care (per hospital protocol). One third of the patients received only standard care.
Of 50 patients treated with calcifediol, one required admission to the ICU (2 percent), while of 26 untreated patients, 13 required admission (50 percent). Of the patients treated with calcifediol, none died, and all were discharged without complications. The 13 patients not treated with calcifediol, who were not admitted to the ICU, were discharged. Of the 13 patients admitted to the ICU, two died and the remaining 11 were discharged.
The study authors suggested that activation of the vitamin D receptor (VDR) signaling pathway may generate beneficial effects in acute respiratory distress syndrome (ARDS) by decreasing the cytokine/chemokine storm; regulating the renin‑angiotensin system; modulating neutrophil activity and by maintaining the integrity of the pulmonary epithelial barrier; stimulating epithelial repair, and tapering down increased coagulability of the blood.
Read more here: https://thevaccinereaction.org/2020/09/three-new-studies-support-vitamin-ds-role-in-preventing-and-treating-covid-19/
Bad Medicine
by Maureen McDonnel | Sep 25, 2020 | COVID-19, Uncategorized
Millions Against Medical Mandates’ Collaborative Communication Committee (comprised of over 30 people from different organizations within our movement) has been generating “packaged messages” in an attempt to reach and influence those unaware of fact-based science regarding vaccine safety and effectiveness. Here is our next message about “bad medicine,” including influenza vaccines. We are asking everyone to review the message below, extract what is relevant for your specific audience, or use the message in its entirety and send it out to your members, family, friends, followers, etc. Please help us push these messages out so more people can wake up to the deeper issues and rise up in solidarity against oppressive and unhealthy directives.
BAD MEDICINE
What is bad medicine? It is both the use of medical interventions that cause more harm than good as well as the failure to use helpful interventions. Moreover, “bad medicine” is the failure to personalize medicine to an individual patient’s needs. With the SARS-CoV-2/COVID-19 crisis that has put our nation – and much of the world – on an unending lockdown, medicine has run amuck.
Why, more than six months into this situation is Anthony Fauci just now mentioning the value of Vitamins C and D, both of which are highly protective for contracting viruses. Why wasn’t he loudly and regularly encouraging every American to protect and boost their immune systems with these widely available inexpensive (hello sunshine and Vitamin D!) vitamins from the very beginning?
Read on to learn more about bad medicine:
- Misuse and overuse of ventilators for COVID-19 patients
- SARS-CoV-2 vaccine trials
- Failure to use effective (and often inexpensive) treatments
- And maybe the biggest “bad medicine” debacle out there – the flu vaccine!
1. Over-Use of Ventilators for COVID-19 Patients was Bad Medicine
Early reports of large percentages of patients dying when placed on ventilators were deeply concerning. Doctors since have learned that not all COVID-19 patients need ventilation, that they were ventilating too many patients, and too soon. Where was the precautionary principle among the panic? https://bit.ly/363aDM3; https://wapo.st/3kJa2TY
2. SARS-CoV-2 Vaccine Trials are Bad Medicine
Many pages could be devoted to issues in the SARS-CoV-2 vaccine trials. Vaccine development is indeed proceeding at warp speed but we need to ask, at what cost? We now have a serious neurological injury –including at least one case and possibly two cases transverse myelitis – in the Oxford/Astra Zeneca trials: https://nyti.ms/2FXcjMB and other significant injuries in the early Moderna trials: https://bit.ly/307MAYB We must demand greater transparency on all injuries to fully understand vaccine risks The most compelling questions are the long and short term potential harms signaled from the clinical trials.
- What impact will messenger RNA (mRNA), used in several vaccine candidates, have on vaccinated people? Even very “pro” mRNA vaccine professionals recognize that there are risks associated with mRNA vaccines – none of which has yet made it to commercial production – including, in particular, the risk of autoimmune diseases (https://go.nature.com/2EzKpFQ) – despite no evidence the public will be screened for autoimmune risks before mass vaccination.
- What about the use of aborted fetal cell lines in the manufacture of several candidate vaccines: https://bit.ly/2G0JVZT? These male and female human DNA cells in various vaccines are being questioned as possible contributors to the exponential rise in gender dysphoria: https://bit.ly/3czcZUq
- What about the use of polyethylene glycol (PEG), a synthetic chemical to which over 70% of people are sensitive –a significant number sensitive to the point of risking anaphylaxis? Moderna has added this dangerous chemical to its vaccine and went so far as to warn its shareholders that the use of PEG was risky to the bottom-line but does not tell clinical trial participants of the risk to them and does not test participants for PEG sensitivity. https://bit.ly/3i2YlWt Not only does PEG carry safety risks, but it may also reduce vaccine efficacy!
- What about risk of antibody-dependent enhancement (or “pathogenic priming”), which creates a possibility that a vaccinated person later exposed to the disease develops far worse symptoms or even dies from a hyper-immune reaction? This risk was seen in animal trials for SARS vaccines years ago and in the recent scandal with Dengvaxia, a dengue fever vaccine, in the Philippines. https://bit.ly/33V6Q0N
- A silver lining here? The distrust surrounding the pharmaceutical industry and government has resulted in Pharma taking the unprecedented step of releasing several trial protocols but we must look at that carefully to determine if these trials were set up for “success” even if the vaccines are not actually safe or effective: https://wb.md/2S9F77f
3. Ignoring or Disparaging Good Medicine is Bad Medicine
The Alliance for Natural Health (ANH-USA) details in their article titled “COVID 411” many specific nutrients that are among the most noteworthy preventives for boosting our immune systems before we get sick. https://bit.ly/2QMBh3d. In particular, a number of therapies and medicines, particularly when combined with zinc, are promising:
- Hydroxychloroquine: https://bit.ly/2ChKtc3; https://bit.ly/3eBTmuf; https://bit.ly/3jbGxtW
- Ivermectin: https://bit.ly/3gSnnqS; https://bit.ly/3hU0GDM; https://bit.ly/32UOn45; https://bit.ly/2YXrWtE
- Quercetin: https://bit.ly/32PwhAh; https://bit.ly/2R1oDxr
- Hinokitiol: https://prn.to/2Z1MalY; https://bit.ly/34W501O
Additionally, there are many other natural treatments and oxidative therapies (using ozone or hydrogen peroxide, for example) that doctors such as David Brownstein, MD, are using with great success: https://bit.ly/34Xz9xA; https://bit.ly/3gQU6Ne. The MATH+ protocol from the Front Line Covid-19 Critical Care (FLCCC) Alliance for severely ill patients is also a good resource: https://bit.ly/3h0Hnrr; https://bit.ly/3bjgOfP.
4. Influenza and Flu Vaccines Shenanigans are Bad Medicine
Del Bigtree really nailed the coffin on flu vaccines on the September 24, 2020 episode of The High Wire, entitled, “Twindemic 2020?” Watch this episode for the most up to date information https://bit.ly/3i3iBqT – the flu issue is addressed beginning around minute 48.
The influenza vaccine’s risk/benefit ratio is high – vaccinating can cause very serious conditions, including neurological harm, autoimmune disease, and death. https://bit.ly/2RYS3wm We also know that getting a flu shot increases your risk of developing more serious non-flu respiratory infections (including some coronavirus infections). https://bit.ly/3ctdbo0 How do we justify the continued push for universal flu shots when the harm outweighs the good?
Yet, the pharmaceutical industry, with its allies in public health and at CDC, present flu as a major cause of death in the U.S., and push flu shots as if they have saved many lives. This information may help put things in perspective:
- Flu shots have caused more bad reactions than all other vaccines combined according to the Vaccine Adverse Events Reporting System (VAERS), and the Vaccine Injury Compensation Program. “Seven out of ten petitions filed between 2016 and 2017 to the NVICP were related to damages following influenza vaccine to adults or children…” https://bit.ly/2G4XFm8
- Flu shots only prevent actual influenza A or B infections, and their effectiveness varies from 10-60% and in most years recently are under 50% effective and often under 30% effective. https://bit.ly/2FRnypY; https://bit.ly/2G4XFm8
- The CDC reported that in the 2018-19 flu season: “Among adults hospitalized for the flu, the vaccine’s effectiveness against the H3N2 strain was reported at -43 percent.” This indicates that those who got their flu shot were more likely to be hospitalized for flu than those who did not get the vaccine! https://bit.ly/2FWKoMM
- A 2009 study by the American Thoracic Society found “…children who had received the flu vaccine [trivalent inactivated flu vaccine—TIV] had three times the risk of hospitalization, as compared to children who had not received the vaccine. In asthmatic children, there was a significantly higher risk of hospitalization [all emphasis mine] in subjects who received the TIV, as compared to those who did not…” This makes the emphasis for asthmatics to take flu shots particularly alarming. https://bit.ly/3ctdMpK
- Over 80% of influenza-like illness – what people generally call “the flu” – are NOT type A or B influenza. They are viral or bacterial flu-like illnesses that are not covered by influenza vaccines. https://bit.ly/2FRnypY
- According to the American Lung Association, flu-caused deaths, as recorded on death certificates over a 13-year period, range between a mere 257-1812 deaths per year in the entire U.S.! https://bit.ly/3652eYD (p.5).
- CDC lumps the pneumonia deaths together with flu deaths, but most pneumonia deaths are unrelated to influenza and therefore could not be prevented or lessened by a flu shot – even if they worked! https://bit.ly/3652eYD
- Universal flu shots violate science and common sense given their high risk to benefit ratio and fact that “Only about 3 percent of pneumonia and influenza deaths occurred in those under age 45.” https://bit.ly/3652eYD (p.6).
CALL TO ACTION:
- Contact FDA and demand transparency in all aspects of the SARS-CoV-2 clinical trials. 1-888-463-6332 Choose option 3 then 1
- Call your governor and state and federal legislators and challenge them on flu vaccine mandates.
- Call vaccine manufacturers and demand transparency.
Read more and take action here: https://mamm.org/bad-medicine/
August News
There is so much going on but the best thing I’ve seen all month is Plandemic Indoctornation. The virus is real, the pandemic is manufactured…this film has documented info… please watch and share! Mom

You can watch both the documentary and see an interview with the director here: https://thehighwire.com/videos/the-highwire-presents-plandemic-indoctornation-2/
Other links to the movie:
https://www.bitchute.com/video/4u7rt61YeGox/https://www.bitchute.com/video/4u7rt61YeGox/
July News
I find it very interesting that the ‘news’ and ‘public health’ sources make all these proclamations but never bother to cite scientific references. All of what they call ‘anti-vaccine’ sites include the links to the actual science.
Always follow the science and follow the money.
Mom
A great series of talks here. Both Dr’s are brilliant and share lots of interesting info. The link is to episode 4, but I do suggest starting at episode 1 and watching them all.
https://disseminate.tv/watch/critically-thinking-with-dr-t-and-dr-p-episode-4_TjkC5BntSkxfv3F.html
Great, brand new film about the 1986 Act that took away liability for vaccine manufacturers. Really important info to watch and share. http://1986theact.com/
The best weekly show I have found for accurate information about what is going on in these crazy times is The Highwire with Del Bigtree. Here’s this weeks show:
Another very interesting video from today, Attorneys Robert F Kennedy jr, and Alan Dershowizt did a vaccine debate this morning. We need to be able to talk about vaccines, vaccine injury and the tobacco science that the companies are using.
That’s this months new. Be well and stand strong. Mom
LOCKDOWN LUNACY: The Thinking Person’s Guide

Great article from the brilliant JB Handley and Children’s Health Defense.
By J.B. Handley, CHD Contributing Writer
For anyone willing to look, there are so many facts that tell the true story, and it goes something like this:
Knowing what we know today about COVID-19’s Infection Fatality Rate, asymmetric impact by age and medical condition, non-transmissibility by asymptomatic people and in outdoor settings, near-zero fatality rate for children, and the basic understanding of viruses through Farr’s law, locking down society was a bone-headed policy decision so devastating to society that historians may judge it as the all-time worst decision ever made. Worse, as these clear facts have become available, many policy-makers haven’t shifted their positions, despite the fact that every hour under any stage of lockdown has a domino-effect of devastation to society. Meanwhile, the media—with a few notable exceptions—is oddly silent on all the good news. Luckily, an unexpected group of heroes across the political landscape—many of them doctors and scientists—have emerged to tell the truth, despite facing extreme criticism and censorship from an angry mob desperate to continue fighting an imaginary war.
My goal is to engage in known facts. You, the reader, can decide if all of these facts, when you put them together, equate to the story above.
Fact #1: The Infection Fatality Rate for COVID-19 is somewhere between 0.07-0.20%, in line with seasonal flu
The Infection Fatality Rate math of ANY new virus ALWAYS declines over time as more data becomes available, as any virologist could tell you. In the early days of COVID-19 where we only had data from China, there was a fear that the IFR could be as high as 3.4%, which would indeed be cataclysmic. On April 17th, the first study was published from Stanford researchers that should have ended all lockdowns immediately, as the scientists reported that their research “implies that the infection is much more widespread than indicated by the number of confirmed cases” and pegged the IFR between 0.12-0.2%. The researchers also speculated that the final IFR, as more data emerged, would likely “be lower.” For context, seasonal flu has an IFR of 0.1%. Smallpox? 30%.
As the first study to peg the IFR, the Stanford study came under withering criticism, prompting the lead researcher, Dr. John Ioannidis to note,
“There’s some sort of mob mentality here operating that they just insist that this has to be the end of the world, and it has to be that the sky is falling. It’s attacking studies with data based on speculation and science fiction. But dismissing real data in favor of mathematical speculation is mind-boggling.”
Like all good science, the Stanford data on IFR has now been replicated so many times that our own Centers for Disease Control came out this week to announce that their ‘best estimate’ showed an IFR below 0.3%. In this article on the CDC’s new data, they also highlighted how the cascading declines in IFR has removed all the fears of doomsday:
That “best estimate” scenario also assumes that 35 percent of infections are asymptomatic, meaning the total number of infections is more than 50 percent larger than the number of symptomatic cases. It therefore implies that the IFR is between 0.2 percent and 0.3 percent. By contrast, the projections that the CDC made in March, which predicted that as many as 1.7 million Americans could die from COVID-19 without intervention, assumed an IFR of 0.8 percent. Around the same time, researchers at Imperial College produced a worst-case scenario in which 2.2 million Americans died, based on an IFR of 0.9 percent.
If you’re still unconvinced that the IFR of COVID-19 is roughly in line with a bad flu season, the most comprehensive analysis I have seen comes from Oxford University, who recently stated:
“Taking account of historical experience, trends in the data, increased number of infections in the population at largest, and potential impact of misclassification of deaths gives a presumed estimate for the COVID-19 IFR somewhere between 0.1% and 0.41%.”
Finally, just last week, Stanford’s Dr. Ioannidis published a meta-analysis (because so many IFR studies have been done around the world in April and early May) where he analyzed TWELVE separate IFR studies and his conclusion is so good, I’ll just leave you with it:
The infection fatality rate (IFR), the probability of dying for a person who is infected, is one of the most critical and most contested features of the coronavirus disease 2019 (COVID-19) pandemic. The expected total mortality burden of COVID-19 is directly related to the IFR. Moreover, justification for various non-pharmacological public health interventions depends crucially on the IFR. Some aggressive interventions that potentially induce also more pronounced collateral harms1 may be considered appropriate, if IFR is high. Conversely, the same measures may fall short of acceptable risk-benefit thresholds, if the IFR is low…Interestingly, despite their differences in design, execution, and analysis, most studies provide IFR point estimates that are within a relatively narrow range. Seven of the 12 inferred IFRs are in the range 0.07 to 0.20 (corrected IFR of 0.06 to 0.16) which are similar to IFR values of seasonal influenza. Three values are modestly higher (corrected IFR of 0.25-0.40 in Gangelt, Geneva, and Wuhan) and two are modestly lower than this range (corrected IFR of 0.02-0.03 in Kobe and Oise).
Opinion #1: Dr. Scott Atlas
Soon after the Stanford study released its data (he wasn’t a study author), Stanford’s Dr. Scott Atlas published an opinion piece in The Hill newspaper with the title, “The data is in — stop the panic and end the total isolation.” He wrote:
The recent Stanford University antibody study now estimates that the fatality rate if infected is likely 0.1 to 0.2 percent, a risk far lower than previous World Health Organization estimates that were 20 to 30 times higher and that motivated isolation policies…Let’s stop underemphasizing empirical evidence while instead doubling down on hypothetical models. Facts matter.
Facts do matter, but no one listened. Dr. Atlas’ article also helps frame Fact #2.
Fact #2: The risk of dying from COVID-19 is much higher than the average IFR for older people and those with co-morbidities, and much lower than the average IFR for younger healthy people, and nearing zero for children
In January 2020, Los Angeles had an influenza outbreak that was killing children, the LA Times noted that “an unlikely strain of influenza has sickened and killed an unusually high number of young people in California this flu season.” COVID-19 is the opposite of that. Stanford’s Dr. Ioannidis said, “Compared to almost any other cause of disease that I can think of, it’s really sparing young people.”
Italy reported three days ago that 96% of Italians who died from COVID-19 had “other illnesses” and were, on average, 80 years old. From Bloomberg:
“The latest numbers show that new cases and fatalities have a common profile: mostly elderly people with previous illnesses,” ISS chief Silvio Brusaferro said at a news conference Friday.
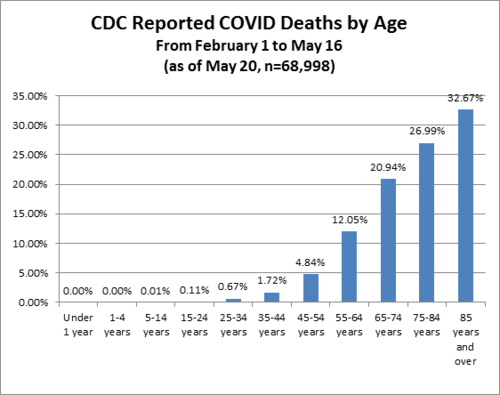
The best age stratification data I have seen comes from Worldometers.info. Here’s their chart estimating death rate by age group. Please note that death rate is MUCH higher than IFR because death rate uses confirmed COVID-19 cases as the denominator, but it shows you how different the fatality rates are by age:
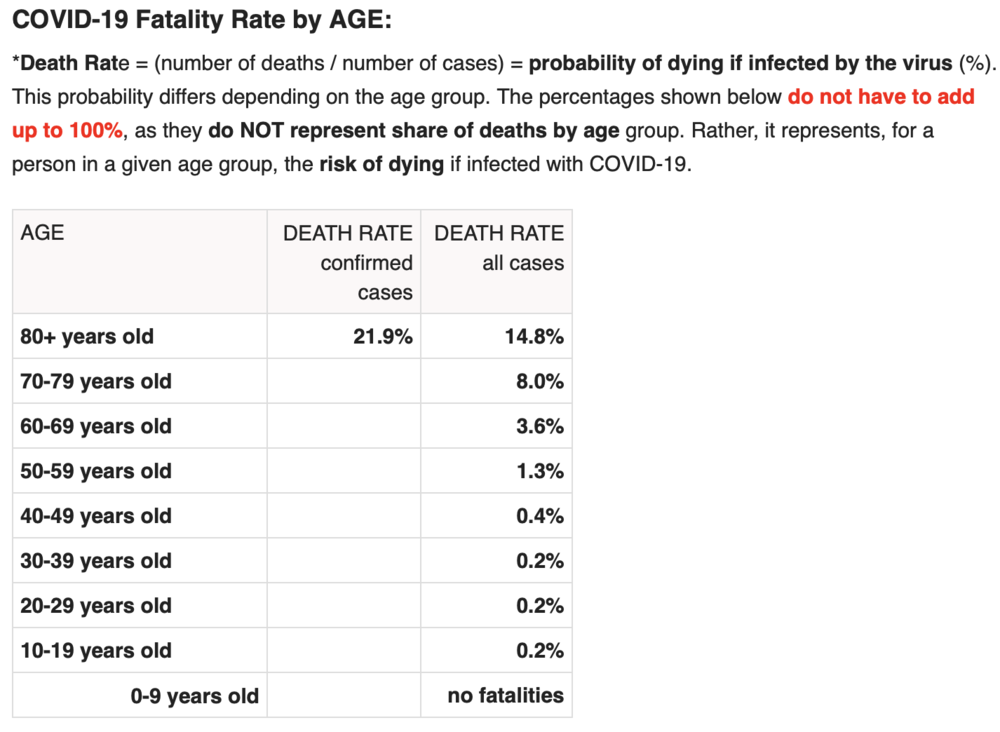
While this data is “crude”, it’s safe to extrapolate that an 80+ year-old person has a serious risk of dying from COVID-19 while a child faces almost no risk. This fact should drive policy, as Dr. Atlas explains:
Of all fatal cases in New York state, two-thirds were in patients over 70 years of age; more than 95 percent were over 50 years of age; and about 90 percent of all fatal cases had an underlying illness. Of 6,570 confirmed COVID-19 deaths fully investigated for underlying conditions to date, 6,520, or 99.2 percent, had an underlying illness. If you do not already have an underlying chronic condition, your chances of dying are small, regardless of age. And young adults and children in normal health have almost no risk of any serious illness from COVID-19.
Consider this excellent article from the British Medical Journal, titled “Shielding from covid-19 should be stratified by risk” written by Cambridge University professors:
Protecting those at most risk of dying from covid-19 while relaxing the strictures on others provides a way forward in the SARS-CoV-2 epidemic, given the virus is unlikely to disappear in the foreseeable future. Such targeted approaches would, however, require a shift away from the notion that we are all seriously threatened by the disease, which has led to levels of personal fear being strikingly mismatched to objective risk of death. Instead, the aim should be to communicate realistic levels of risk as they apply to different groups, not to reassure or frighten but to allow informed personal decisions in a setting of necessary uncertainty.
As one simple example: closing schools makes almost no sense given what we know about COVID-19, while protecting teachers over the age of 60—to pick a somewhat defensible age boundary—may well make sense. This is why so many countries who seem to respect data more than we do here in the U.S. have already re-opened their schools. In fact, Denmark’s schools have been open since mid-April!! And, for those keeping score, Reuters just reported yesterday that, “Reopening schools in Denmark did not worsen outbreak, data shows.” Here’s a quote:
“You cannot see any negative effects from the reopening of schools,” Peter Andersen, doctor of infectious disease epidemiology and prevention at the Danish Serum Institute said on Thursday told Reuters. In Finland, a top official announced similar findings on Wednesday, saying nothing so far suggested the coronavirus had spread faster since schools reopened in mid-May.
Another great article on schools, titled, “It is fear – not science – that is stopping our children being educated” in The Telegraph newspaper last week, here’s a quote:
There is little about coronavirus we can be absolutely sure of – this is a brand new disease and our knowledge grows by the day – but most of the available evidence so far strongly suggests that children are neither suffering from coronavirus nor spreading it. Studies in South Korea, Iceland, Italy, Japan, France, China, the Netherlands and Australia all concur that youngsters are “not implicated significantly in transmitting Covid”, not even to parents and siblings.
Adult paranoia, stoked by over-the-top government messaging, union intransigence and media conniptions, is now being inflicted on the youngest members of our society to whom the virus poses a threat so tiny scientists call it “statistically irrelevant”. Instead of nursery rhymes, mixed infants may soon be invited to sing something called the “two-metre-song” as they stick their arms out to keep their friends at bay.
Brand new science (May 28) released from Northern Ireland clearly shows that schoolchildren do NOT serve as vectors for COVID-19. Titled, No evidence of secondary transmission of COVID-19 from children attending school in Ireland, 2020, the study could not be more clear:
These findings suggest that schools are not a high risk setting for transmission of COVID-19 between pupils or between staff and pupils. Given the burden of closure outlined by Bayhem [4] and Van Lanker [5], reopening of schools should be considered as an early rather than a late measure in the lifting of restriction.
Finally, Dr. Scott Atlas took on the topic of schools in this recent interview:
“There’s no science whatsoever to keep K-through-12 schools closed, nor to have masks or social distancing on children, nor to keep summer programs closed. What we know now is that the risk of death and the risk of even a serious illness is nearly zero in people under 18.
Quick update: after I wrote this, the Wall Street Journal published this article titled Is It Safe to Reopen Schools? These Countries Say Yes. To me, this reads as a bit of a litmus test for countries that have independent and data-driven public health officials, and I give the U.S. an ‘F” for our current approach:
But Denmark, Austria, Norway, Finland, Singapore, Australia, New Zealand and most other countries that have reopened classrooms haven’t had outbreaks in schools or day-care centers…In Denmark, the opening of schools had no impact on the progress of the epidemic, said Tyra Grove Krause, a senior official with the State Serum Institute, the country’s disease control agency…Since Austria reopened on May 18, no increase in infections has been observed in schools and kindergartens, a spokesman for the government said…In Norway, the government won’t close schools again even if the number of cases starts rising in the country because there have been no negative consequences from reopening schools on April 20, said Education Minister Guri Melby.
How many more countries need to re-open before the U.S. follows? Seriously, it’s a little embarrassing to be American…IMO we look like total chumps.
Update #2: Dr. Scott Atlas doubled-down on June 1st with this great Op-Ed, once again in The Hill, titled Science says: ‘Open the schools’. As usual, he’s amazingly eloquent, here’s an excerpt but well worth the time to read every word, he simply slays it:
All of this borders on the absurd, when we now know that social distancing and face coverings for children are completely unnecessary.
Never have schools subjected children to such an unhealthy, uncomfortable and anti-educational environment, so science cannot precisely define the total harm it will cause. But science does tell us that risks from COVID-19 are too minimal to sacrifice the educational, social, emotional and physical well-being – to say nothing of the very health – of our young people.
(Special note: there’s a new boogeyman, Kawasaki disease, that some are trying to link to COVID-19. Here’s a great article about that, or see the website of the UK’s Kawasaki Disease Foundation where they discuss the “mishandling of information” about Kawasaki disease. Dr. Atlas’ most recent post discusses this, too: “What about the new threat similar to Kawasaki disease, recently sensationalized as a COVID-19 association? In fact, the association is extremely low, and the incidence of the disorder is itself rare, affecting only 3,000 to 5,000 children in the United States each year. Importantly, the syndrome is typically treatable and never has been regarded previously as a risk so serious that schools must be shuttered.”)
Fact #3: People infected with COVID-19 who are asymptomatic (which is most people) do NOT spread COVID-19

On January 13, 2020, a 22-year old female with a history of congenital heart disease went to the emergency room of Guangdong Provincial People’s Hospital complaining of a variety of symptoms common to people with her condition, including pulmonary hypertension and shortness of breath due to atrial septal defect (hole in the heart). Little did she know her case would set off a cascade of events resulting in a recently published paper that should have ended all lockdowns around the world simultaneously. Three days into her hospital stay, her condition was improving. Routine tests were run, and to the clinicians alarm and surprise, she tested positive for COVID-19. As the physicians noted, “the patient had never fever, sore throat, myalgia or other symptoms associated with virus infection.” Said differently, she was completely asymptomatic for COVID-19.
It’s not that easy to find people who are infected with COVID-19 but asymptomatic, because they don’t seek medical attention. Here in Oregon where I live, you can’t even get a COVID-19 test unless you have symptoms. So, the stars aligned to put this woman in a hospital with researchers studying COVID-19, and she became the subject of an extensive contact study published on May 13 in Respiratory Medicine, titled, “A study on infectivity of asymptomatic SARS-CoV-2 carriers.”
The researchers wanted to find out whether this woman, with a COVID-19 infection but no symptoms, had infected anyone else, so they chose to look at every single contact they could identify within the previous 5 days prior to her positive test. So, how many people did they have to screen? 455. Not a small number, as the researchers explain:
455 contacts who were exposed to the asymptomatic COVID-19 virus carrier became the subjects of our research. They were divided into three groups: 35 patients, 196 family members and 224 hospital staffs. We extracted their epidemiological information, clinical records, auxiliary examination results and therapeutic schedules.
As you can see, being hospitalized led to the majority of the contacts this woman had, both with other patients and with many members of the hospital staff. Notably, all of these contacts took place indoors and one might argue many of the contacts—at least with hospital staff—would have involved relatively intimate contact. Amongst the patients, the average age was 62, arguably making them higher risk, and many of those patients were immunocompromised for a variety of reasons, including chemotherapy and cardiovascular disease. So how many of the 455 people were infected by the asymptomatic 22-year old woman?
“In summary, all the 455 contacts were excluded from SARS-CoV-2 infection…”
Said differently, exactly zero people were infected. The scientists, in typically understated fashion, offer up a comment about the question I hope you are asking yourself right now (namely, why are we all on lockdown if asymptomatic people with COVID-19 can’t spread the infection?), stating, “the result of this study may alleviate parts of the public concern about asymptomatic infected people.”
If this study had been published in early March, the odds that the world would have locked down are very, very low. Yet, this study, published only two weeks ago, is nowhere to be found in the media, and is never mentioned by policy makers. It just sits there, sharing the truth for anyone willing to listen.
Fact #4: Emerging science shows no spread of COVID-19 in the community (shopping, restaurants, barbers, etc.)
“There is no significant risk of catching the disease when you go shopping. Severe outbreaks of the infection were always a result of people being closer together over a longer period of time…”
– Professor Hendrick Streek , University of Bonn
We just learned that asymptomatic people infected with COVID-19 are very unlikely to be able to spread the infection to others. Emerging and published science shows transmission of COVID-19 in retail establishments is extremely unlikely. Professor Hendrik Streeck from the University of Bonn is leading a study in Germany on the hard-hit region of Heinsberg and his conclusions, from laboratory work already completed, is very clear:

“There is no significant risk of catching the disease when you go shopping. Severe outbreaks of the infection were always a result of people being closer together over a longer period of time.
“When we took samples from door handles, phones or toilets it has not been possible to cultivate the virus in the laboratory on the basis of these swabs….”
Uh oh. You mean closing parks, closing stores, wearing gloves and masks at the grocery store, fumigating our groceries, and just being generally paranoid wasn’t necessary? As Dr. Streeck confirms:
“It is important to obtain this data in order to make sure that decisions are taken based on facts rather than assumptions. The data should serve as a basis of information for the government so they can then think about their further course of action,” he said.
And he continues:
“People could lose their jobs. They might not be able to pay their rent anymore and staying inside for a longer time can lead to weakening of our immune system.”
“The goal is not a complete containment of the virus. We need to know where the actual capacity limits of our hospitals are. How many infections are too many? What do intensive care medics say?”
And, finally:
“It is important to start thinking about a ‘rollback’ strategy and his hope is to “deliver the relevant facts so that people have a good foundation for their decisions.”
Fact #5: Published science shows COVID-19 is NOT spread outdoors

In a study titled Indoor transmission of SARS-CoV-2 and published on April 2, 2020, scientists studied outbreaks of 3 or more people in 320 separate towns in China over a five-week period beginning in January 2020 trying to determine WHERE outbreaks started: in the home, workplace, outside, etc.? What’d they discover? Almost 80% of outbreaks happened in the home environment. The rest happened in crowded buses and trains. But what about outdoors? The scientists wrote:
“All identified outbreaks of three or more cases occurred in an indoor environment, which confirms that sharing indoor space is a major SARS-CoV-2 infection risk.”
Said differently, there’s really no science to support all the outdoor bans that my home state of Oregon and so many other states have put in place. I’ll leave you with my favorite quote from the study because it’s really quite infuriating to read when you consider some of the ways Governors here in the U.S have behaved (and some still do) by banning all sorts of outdoor activities, arresting paddle boarders on the water, etc.:
“The transmission of respiratory infections such as SARS-CoV-2 from the infected to the susceptible is an indoor phenomenon.”
Quick Update: Apparently the health minister of British Columbia, Canada, got the memo about the lack of airborne risk, this article appeared on June 1:

One of B.C.’s top health officials, however, says medical professionals have a pretty clear picture of how the virus is transmitted. “There is absolutely no evidence that this disease is airborne, and we know that if it were airborne, then the measures that we took to control COVID-19 would not have worked,” Dr. Reka Gustafson, B.C.’s deputy provincial health officer, told CTV Morning Live Monday.”We are very confident that the majority of transmission of this virus is through the droplet and contact route….”The overwhelming majority of (COVID-19) transmissions occur through close, prolonged contact and that is not the pattern of transmission we see through airborne diseases,” she said.
I sure hope Major League Baseball, the National Football League, and the NCAA are all paying attention…not to mention all the people in Portland here still riding bikes and running with masks on.
Fact #6: Science shows masks are ineffective to halt the spread of COVID-19, and The WHO recommends they should only be worn by healthy people if treating or living with someone with a COVID-19 infection
May 29th, the World Health Organization announced that masks should only be worn by healthy people if they are taking care of someone infected with COVID-19:
“If you do not have any respiratory symptoms such as fever, cough or runny nose, you do not need to wear a mask,” Dr. April Baller, a public health specialist for the WHO, says in a video on the world health body’s website posted in March. “Masks should only be used by healthcare workers, caretakers or by people who are sick with symptoms of fever and cough.”
Just before the COVID-19 madness, researchers in Hong Kong submitted a study for publication with the mouthful of a title, “Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings—Personal Protective and Environmental Measures.” Oddly, the study, just published this month, is actually housed on the CDC’s own website, and directly contradicts recent advice from the CDC about wearing a mask. Namely, the study states:
“In our systematic review, we identified 10 RCTs that reported estimates of the effectiveness of face masks in reducing laboratory-confirmed influenza virus infections in the community from literature published during 1946–July 27, 2018….In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks…Our systematic review found no significant effect of face masks on transmission of laboratory-confirmed influenza….Proper use of face masks is essential because improper use might increase the risk for transmission.”
English translation: there is no evidence that wearing masks reduces the transmission of respiratory illnesses and, if masks are worn improperly (like when people re-use cloth masks), transmission could actually INCREASE. Moreover, this study was a meta-analysis, which means it dug deep into the archive of science (all the way back to 1946!) to reach its conclusions. Said differently, this is as comprehensive as science gets, and their conclusions were crystal clear: masks for the general population show no evidence of working to either slow the spread of respiratory viruses or protect people.
This study is far from the only one to reach this conclusion (which makes the choice of a grocery store chain like my beloved New Seasons to make masks mandatory for all customers really quite unbelievable). The purpose of science is to arbitrate these thorny issues and while the science is clear, the hysteria continues. It turns out, the effectiveness of masks has a long history of debate in the medical community, which explains why so much science has been done on the topic. I will just highlight a few studies before you fall asleep:
My favorite article is actually a review of much of the science and it’s a great place to start for anyone who likes to do their own research. Titled, “Why Face Masks Don’t Work: A Revealing Review”, it was written to challenge the need for dentists to wear face masks, but all the science quoted and conclusions drawn apply to airborne pathogens in any setting. Some of the best quotes:
“The science regarding the aerosol transmission of infectious diseases has, for years, been based on what is now appreciated to be ‘very outmoded research and an overly simplistic interpretation of the data.’ Modern studies are employing sensitive instruments and interpretative techniques to better understand the size and distribution of potentially infectious aerosol particles…The primary reason for mandating the wearing of face masks is to protect dental personnel from airborne pathogens. This review has established that face masks are incapable of providing such a level of protection.”
And my favorite quote:
“It should be concluded from these and similar studies that the filter material of face masks does not retain or filter out viruses or other submicron particles. When this understanding is combined with the poor fit of masks, it is readily appreciated that neither the filter performance nor the facial fit characteristics of face masks qualify them as being devices which protect against respiratory infections. ”
Here’s an article published in ResearchGate by noted Canadian physicist D.G. Rancourt, written directly in response to the COVID-19 outbreak, published last month. Titled, Masks Don’t Work: A review of science relevant to COVID-19 social policy.
“Masks and respirators do not work. There have been extensive randomized controlled trial (RCT) studies, and meta-analysis reviews of RCT studies, which all show that masks and respirators do not work to prevent respiratory influenza-like illnesses, or respiratory illnesses believed to be transmitted by droplets and aerosol particles. Furthermore, the relevant known physics and biology, which I review, are such that masks and respirators should not work. It would be a paradox if masks and respirators worked, given what we know about viral respiratory diseases: The main transmission path is long-residence-time aerosol particles (< 2.5 μm), which are too fine to be blocked, and the minimum-infective-dose is smaller than one aerosol particle.”
To put this in simple terms: in order for a mask to really be effective that covered both your nose and mouth, you would asphyxiate. The minute the mask allows you to breathe, it can no longer filter the micro-particles that make you sick.
Finally, I often see this study from 2015 in the BMJ cited: “A cluster randomised trial of cloth masks compared with medical masks in healthcare workers“, and it bears repeating, since MOST of the masks I see people wearing in the community right now are cloth masks. Not only are these masks 100% ineffective at reducing the spread of COVID-19, but they can actually harm you. As the researchers explain:
“This study is the first RCT of cloth masks, and the results caution against the use of cloth masks. This is an important finding to inform occupational health and safety. Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection. Further research is needed to inform the widespread use of cloth masks globally.”
Increased risk of infection? Yes, that’s what it says. Other studies have also looked at the impact masks have on your oxygen levels (because you’re are forced to re-breathe your own Co2) and it’s not good. Scientists looked at oxygen levels of surgeons wearing masks while performing surgery and found: “Our study revealed a decrease in the oxygen saturation of arterial pulsations (SpO2) and a slight increase in pulse rates compared to preoperative values in all surgeon groups.”
Just this past week, this article came out in the New England Journal of Medicine, written my several doctors and public health officials with the title, “Universal Masking in Hospitals in the Covid-19 Era,” and this statement seems a perfect way to end my discussion of masks:
We know that wearing a mask outside health care facilities offers little, if any, protection from infection. Public health authorities define a significant exposure to Covid-19 as face-to-face contact within 6 feet with a patient with symptomatic Covid-19 that is sustained for at least a few minutes (and some say more than 10 minutes or even 30 minutes). The chance of catching Covid-19 from a passing interaction in a public space is therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic.
Read the rest here: https://childrenshealthdefense.org/news/lockdown-lunacy-the-thinking-persons-guide/
PlanDemic, a film about the global plan to take control of our lives, liberty, health & freedom
Really good information here, by Dr. Judy Mikovits and others.
YouTube is censoring. The clip (25 minutes) had over a million views. You can download it free from their site.
Petition: Repeal Immunity for Drug Companies Against Vaccine Injuries
Please sign and share! xo Mom
Repeal Immunity for Drug Companies Against Vaccine Injuries
Why should the drug companies be above the law? If vaccines are safe, there would be no need to grant the drug companies immunity. In 1986 Congress gave the drug companies immunity against all lawsuits from vaccine related injuries. The Federal Government is now paying out billions in damages to some parents whose children have been hurt by vaccines. While the drug companies continue to rack up huge profits, most families continue to pay for the damages with their own money.
Why is this important?
This petition was started by a citizen and not by MoveOn. Please ask Moveon to support this petition by clicking on the link in the red banner above.
NEW: HHS has not done ANY vaccine safety studies for 32 years as required by the 1986 law.
Please share this important information with your
doctor/nurse and legislators at the local and federal level.
—————————————————————–
NEW: Injury/Death Stats from all vaccines since 1987 is given below.
This information is publicly available from https://www.medalerts.org/vaersdb/findfield.php.
Please do your own search. It is very easy!
The number of deaths from all vaccines since 1987 is 5,726. The number of people disabled from all vaccines since 1987 is 13,718. The number of people hospitalized after a vaccine is 59,368. The number of ER visits is 180,476.
And we are told that vaccines are completely safe for
everyone!
—————————————————————————–
In 1986 Congress granted immunity to vaccine makers against all lawsuits. This
is blatantly unfair and un-American. No other industry group is protected in
this manner. People in other countries can sue vaccine makers and do but we in
America cannot! The US Government is now grudgingly paying billions to parents
of children damaged by vaccines, but only after years of litigation. Only 1 in
5 claimants ever gets paid. This, at a time when the vaccine makers such as
Merck make billions in profits. Sound familiar? Corporate socialism! The
compensation money comes from a $0.75 excise tax that vaccine makers pay for
each shot but this is hardly adequate. Families are often burdened with
thousands of dollars each year to take care of vaccine injured (sometimes
permanently) children. The maximum payout is capped at $250K if a child dies.
Clearly Congress decided to serve the corporations rather than the people! THIS
HAS TO STOP. NOW!
The vaccine makers continue to make more vaccines and are lobbying state legislatures to remove existing personal and religious exemptions (e.g. SB 277 and SB 792 in CA). There is talk of making vaccination mandatory for adults also. Immunity from prosecution for vaccine manufacturers must be repealed because with immunity, vaccine makers have no incentive to make sure vaccines are safe. We want better and safer vaccines. This will happen ONLY if we repeal vaccine manufacturers’ immunity.
Vaccine makers cannot lobby/pay politicians to force mandates on our kids, grand kids and on us and not pay for the damages their products cause! Our medical freedoms are paramount and no government should force us to inject chemicals into our bodies without our consent! Not in the LAND OF THE FREE!!
WE NEED YOUR HELP TO SHARE THIS WITH YOUR COLLEAGUES, FRIENDS AND FAMILY. PLEASE MAKE THIS CAUSE YOUR OWN. TOGETHER, WE CAN GET OUR RIGHTS BACK!! Please comment if you may.
Please watch/read and decide for yourself if vaccines are safe or not.
1. https://vimeo.com/126792405
2. http://vaxxedthemovie.com/
3. http://www.thevaccinereaction.org/2016/04/robert-de-niro-debates-autisms-link-to-vaccines-today-2/
4. http://www.boughtmovie.net/free-viewing/
5. https://vactruth.com/2016/06/03/vaccinated-vs-unvaccinated/
6. http://avoiceforchoice.org/
Vaccines in the news
Where to even start this month, while the world is in lock down. Just dropping some of the best articles I’ve found, as links below. Stay well. Mom
RKF jr. on Gates
RFK jr. on the Flu vaccine
Researchers say Californians may have developed herd immunity to coronavirus. Yet researchers at Stanford University have theorized that coronavirus first hit California undetected last year, much earlier than anyone realized, and was only seen at that time as a particularly nasty and early flu season. (I know so many people who were seriously sick then)
https://abc7chicago.com/herd-immunity-coronavirus-california-stanford/6092370/
Also this is really important from Web MD and a NY doctor who’s been on the front lines. They are finding that the patients being put on respirators are dying, possibly from the respirators – they need oxygen (like masks) but not respirators. And that’s it’s doesn’t seem like pneumonia, but actually is appearing more like altitude sickness which would just require oxygen.
https://www.webmd.com/lung/news/20200407/doctors-puzzle-over-covid19-lung-problems
Here’s the interview:
https://www.webmd.com/coronavirus-in-context/video/coronavirus-in-context-cameron-kyle-sidell
Corona Virus Vaccine info……
They are going ahead with human trials in Washington State, AND skipping the animal studies that should be done beforehand (and as usual, no placebo testing.)
From the article:
Studies have suggested that coronavirus vaccines carry the risk of what is known as vaccine enhancement, where instead of protecting against infection, the vaccine can actually make the disease worse when a vaccinated person is infected with the virus. The mechanism that causes that risk is not fully understood and is one of the stumbling blocks that has prevented the successful development of a coronavirus vaccine.
Read more here:
Dr. Toni Bark
The world has lost an incredible voice this week. Dr. Toni Bark. She was a Pediatrician, the former head of a pediatric ER in the Chicago area and was a much honored doctor. Please watch. Mom
Imagine if there was proof that vaccines weren’t safe…
Unfortunately, there is… Mom
Study: For 1 in 168 children, vaccines cause side effects so severe that they require an ER visit.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3236196/
Study: Boys vaccinated against Hep B at birth are 3x more likely to develop autism.
http://www.ncbi.nlm.nih.gov/pubmed/21058170
Analysis: SIDs and Infant Mortality Rates Regressed Against Number Of Vaccine Doses Routinely Given “A high statistically significant correlation between increasing number of vaccine doses and increasing infant mortality rates…”
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3170075/
Case Study: Rare simultaneous Sudden Infant Death (SID) of identical twins 2 days after vaccination.
https://www.ncbi.nlm.nih.gov/pubmed/17654772
Study: Rotovirus linked to fatal intestinal disorder in 1 in every 4670 infants. “There was also an increase in the risk of intussusception after the second dose of the vaccine… The strong association between vaccination with RRV-TV and intussusception among otherwise healthy infants supports the existence of a causal relation.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1773072/
Study: “Epidemiological evidence supporting an association between… Thimerosal-containing childhood vaccines and the subsequent risk of an ASD diagnosis.”
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3878266/
Study: “The higher the proportion of children receiving recommended vaccinations, the higher was the prevalence of AUT or SLI. A 1% increase in vaccination was associated with an additional 680 children having AUT or SLI. Neither parental behavior nor access to care affected the results, since vaccination proportions were not significantly related (statistically) to any other disability or to the number of pediatricians in a U.S. state. The results suggest that although mercury has been removed from many vaccines, other culprits may link vaccines to autism.”
http://www.ncbi.nlm.nih.gov/pubmed/21623535
Analysis: “The risk of autism among African American children vaccinated before the age of 2 years was 340% that of those vaccinated later.”
http://www.ncbi.nlm.nih.gov/pubmed/25377033
Analysis: “Methodological issues and evidence of malfeasance in research purporting to show thimerosal in vaccines is safe.”
http://www.ncbi.nlm.nih.gov/pubmed/24995277
Study: Link between antibodies from MMR vaccine and central nervous system autoimmune dysfunction in children with autism
http://www.ncbi.nlm.nih.gov/pubmed/12145534
Study: Link between aluminum in vaccines and prevalence of autism
http://www.ncbi.nlm.nih.gov/pubmed/22099159
Study: “The related and damaging effect of exposure to high levels of mercury… a viable alternative explanation for the occurrence of regressive autism. The evidence indicates there is alteration to chromosome structure and/or function.”
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3364648/
Case Series: Vaccine additives cause autism-like symptoms.
http://www.ncbi.nlm.nih.gov/pubmed/17454560
Analysis: “A comprehensive review of mercury-provoked autism. In conclusion, the overwhelming preponderance of the evidence favours acceptance that Hg exposure is capable of causing some ASDs.”
http://www.ncbi.nlm.nih.gov/pubmed/19106436
Analysis: Explanation of why some children are at greater risk of developing autism after vaccines. “The evidence suggests that the abnormal sulfation chemistry, limited thiol availability, and decreased GSH res
A Shot in the Dark
Very good short documentary. Watch and share! Mom